

Effective public health messaging for adverse weather events
Research completed December 2025
DOI: https://doi.org/10.7488/era/7268
Executive summary
Our research examines effective approaches for delivering persuasive messages that support protective health behaviours during adverse weather events. We focus on four weather events within Public Health Scotland’s Adverse Weather and Health Plan 2024–27: periods of hot and cold weather, flooding and drought.
We investigate evidence on the effectiveness of public health messages disseminated for adverse weather events, for general and at-risk populations; which communication channels are most effective; and factors that influence the public’s risk perception and health and wellbeing behavioural responses in relation to adverse weather.
This study was delivered in two phases: a Rapid Evidence Review, supplemented by an engagement phase with organisations representing groups at heightened risk from adverse weather in Scotland.
Findings
Effectiveness of public health messages
Evidence on the effectiveness of public health communication disseminated for adverse weather is limited. Few studies directly link communication to health outcomes, with most focusing on intermediate outcomes such as awareness, knowledge, and behaviour change or intentions to act.
Only three international studies provide causal evidence on the effectiveness of communication interventions specifically designed to target vulnerable populations (older adults, people with chronic conditions). All three focus on heat. From these studies, we learned that:
- Public health messages can lead to behaviour change including improvements in health and reduced pressure on health services.
- Complementary policy interventions can enhance impact of communications, enabling behaviour change even in the absence of increases in awareness or knowledge of health risks – highlighting that these are not always necessary preconditions for action.
- Targeted information can improve health and behaviour, but some sub‑groups may benefit more than others.
Four studies examine public responses to general heat-health messaging delivered through campaigns and alerts in ‘real-world’ settings. Across these studies, the relationship between exposure to advice and self-reported behaviour change is not consistent. Hearing public health information is associated with stronger intentions to act for some individuals, but effects can be modest and uneven, or concentrated in particular groups, and some of those most likely in need of protection are less likely to act. Rather than reflecting a simple linear relationship between information and action, this evidence points to a more complex picture in which behavioural responses are shaped by multiple factors that communicators need to consider.
Factors influencing perception and behavioural responses to adverse weather
The majority of studies we found offer insights into the factors shaping how people perceive, interpret, and respond to adverse weather risks. This evidence suggests that behavioural responses emerge from the interaction of multiple influences. Consistent patterns emerge:
- Personal experience of adverse weather can increase receptivity to guidance. Lack of prior experience, particularly relevant for drought in Scotland, weakens risk perception.
- Efficacy beliefs: confidence that recommended protective actions are effective (response efficacy) and achievable (self-efficacy) consistently emerge among the strongest predictors of adaptive behaviour. However, practical barriers such as cost, housing conditions, physical capability, and access to resources can constrain people’s ability to act even when they recognise risks.
- Emotions can influence protective intentions. Positive associations to warm weather, particularly relevant to heat and drought, can weaken perceptions in the UK context, while fear or concern alone do not necessarily lead to protective action unless people also feel capable of responding effectively.
- Socio-demographic and socio-economic factors do not reliably predict how people perceive weather-related health risks or their behavioural responses. Structural factors, including cost, housing conditions, physical capacity, digital access, literacy, and language, influence whether people receive, interpret, and feel able to act on advice.
- Social and cultural environments, including prevailing norms, collective narratives about weather, and trusted relationships with messengers, shape how people interpret advice and whether they act on it.
Principles for effective messaging
- Make guidance actionable, specific, and directive – people need to believe they are capable of the action and that it will be effective
- Ensure ‘message relevance’: people need to see themselves in the message and believe the message is for them. This includes being mindful of how people self-identify and supporting people to personalise the risk.
- Consider people’s emotional responses to certain weather events as some e.g. heat and drought can attract positive emotions. However, counteracting these with negative framings is insufficient unless combined with efficacy information.
- Communication should be tailored to different audiences, recognising variation in language, literacy, housing conditions, income, geography, and other factors that shape how people access, interpret, and act on information
- Clear, inclusive, and accessible language can improve engagement. Visuals, infographics, storytelling, and culturally relevant communication approaches can further support understanding and make messages feel more personally relevant.
- Timing relevant to the weather event is important.
Effective communication channels
We found no studies that compare which communications channels or messengers are most effective in influencing changes in awareness, knowledge, attitudes or behaviours. 21 studies across heat (12), drought (3) floods (2), and mixed hazards (4) provide evidence on the main channels used to disseminate information, patterns of access and preference, and the relative strengths and limitations in terms of reach and accessibility. Some of the studies provide insights into characteristics and design features of particular channels such as websites and social media. Broad patterns and principles of effective communication channels emerge:
- Traditional channels (broadcast and print media) remain widely used and valued, especially among groups less likely to engage online.
- Digital channels, including websites and social media, are important components of adverse-weather communication strategies. Websites are widely used sources of information, while social media platforms are increasingly used to disseminate adverse-weather and health information and may help reach audiences less likely to engage with traditional media, particularly younger groups. However, access, engagement, and audience reach are uneven.
- Formal and informal community networks are particularly important for those who may not engage with formal or digital channels. Their effectiveness is underpinned by credibility and trust; amplification and reach; and relevance and personalisation.
Cross-cutting principles of effective communication channels
- Diversify channels for maximum reach and exposure.
- Design for equity, reflecting differences in preferences and access patterns, which vary by digital connectivity, literacy, language, and cultural context.
- Ensure consistency across channels and messengers. When messages differ across sources or channels, they can cause confusion and reduce trust and compliance.
- Trust in the source matters.
Links to the wider evidence
Our findings align well with the wider evidence based on public health communication and risk perception but deliver important nuance on communicating public health advice in relation to extreme weather events. For example, on the importance of combining appeal to emotions with efficacy cues.
Glossary / Abbreviations
Adverse weather | “Weather events such as episodes of hot or cold weather or flooding from heavy rainfall, that have an impact on public health and wellbeing. The level at which risks to health start to increase are not necessarily severe or extreme”. (UK Health Security Agency, 2024 p. 11) |
AWHP | Adverse Weather and Health Plan |
Emergency management | Emergency management is the process to plan for, respond to and recover from risks. It involves: assessing the risks and available resources to respond; prevention – reducing risks and their impacts; preparation – planning response to the risk; responding to the situation; recovery – achieving a return to normality and identifying lessons to develop and improve for future emergencies. In Scotland, this involves partners working together in what is called Integrated Emergency Management. Source: The foundations of emergency management in Scotland (Lesson 4 – the resilience cycle – Ready Scotland) |
Extreme weather | “Exceptionally adverse, severe, unusual or unexpected weather conditions for the season and location”. (UK Health Security Agency, 2024 p. 11) |
GP | General Practitioner |
LLSI | Limiting long-standing illnesses |
Meta-analysis | A method of synthesis of quantitative data from multiple independent studies addressing a common research question. |
PMT | Protection Motivation Theory |
Quasi experimental study | A study design assesses the impact of an intervention using comparison groups but without randomly assigning participants to those groups (as a Randomised controlled trial would, see below). |
RCT | Randomised controlled trial. A study design that assesses the impact of an intervention by randomly assigning participants to different groups (for example, an intervention group and a comparison group), allowing stronger conclusions about whether the intervention caused the observed outcomes. |
RER | Rapid Evidence Review. A streamlined, time-efficient method for synthesising existing research to inform decision-making, by adapting traditional systematic review processes to a shorter timeline, focusing on key literature rather than being exhaustive, while maintaining transparency and rigour. |
Scoping review | A structured approach to evidence synthesis that identifies, organises, and describes the breadth of research available on a particular topic or field. It is typically undertaken where the evidence base is emerging, heterogeneous, or has not yet been comprehensively reviewed. Its primary purpose is exploratory: to map the range, nature, and volume of existing evidence, clarify key concepts and definitions, and identify gaps where further research may be required. |
Severe weather | “Any destructive weather conditions that increase the risk of harm to public health and wellbeing, with impacts being felt across sectors”. (UK Health Security Agency, 2024 p. 11) |
SNAP3 | Scottish National Adaptation Plan |
Systematic Review | A type of evidence or literature review that uses a highly structured methodology that identifies, appraises, and synthesises all available high-quality evidence on a specific research question. |
UK | United Kingdom |
Introduction
Background: the need for this research
Average temperatures in Scotland are rising, and climate change is contributing to more frequent episodes of heat and cold, flooding and drought, all of which have implications for public health and health inequalities (Adaptation Scotland, 2025; Climate Change Committee, 2021; James Hutton Institute, 2023, Sayers et. al, 2023; UK Health Security Agency, 2023, 2024).
Scotland has a comprehensive policy framework to address the health impacts of climate change. The Scottish Government has developed a set of climate resilience policies, including Climate Ready Scotland, the Climate Change Plan, and the Just Transition Plan. The national response to climate risks is coordinated through the Scottish National Adaptation Plan 2024–2029 (SNAP3).
One important deliverable within SNAP3 is the Public Health Scotland (PHS) Adverse Weather and Health Plan 2024–27 (AWHP), published in July 2024 (PHS, 2024). The Plan sets out PHS’s commitment to working with partners to help mitigate, prepare for, and respond to the potential health risks associated with adverse weather, also recognising that these risks fall unequally across the population. The Plan covers the following weather-related hazards, with a significant impact on health: heat, cold, flooding, and drought.
There is a strong evidence base demonstrating that periods of hot or cold weather, flooding and other adverse weather events pose substantial effects on population health and wellbeing (UK Health Security Agency, 2023). As the AWHP highlights, these impacts are wide-ranging and, to a large extent, preventable. Health effects arise through both direct exposure and wider indirect pathways, with consequences that can be immediate or persist over time. They can exacerbate existing health problems and can contribute to illness, disability, or premature death (PHS, 2024).
While exposure to adverse weather can affect anyone, some people may be more affected than others, due to a wide range of factors, including but not limited to, age, underlying health status, geographical location and socioeconomic status.
The AWHP highlights effective communication as an important component of supporting resilience and preparedness, emphasising the need for messages that are inclusive, accessible, and responsive to different needs and circumstances. However, whether and how people adopt health-protective behaviours in response to communications about adverse weather is complex. People’s perceptions of the risks and their behavioural responses are shaped by a wide range of psychological, social, cultural, and structural factors (Spielhofer et al, 2020). Understanding these influences and communicating effectively, with all the complexities in mind, is critical.
Our research examines effective approaches for delivering persuasive messages that support protective health behaviours during adverse weather events, focusing specifically on the four weather events within the AWHP.
Research aims and report structure
The overall purpose of the research is to help support the delivery of the AWHP 2024-27. It aims to establish the most relevant and effective communication approaches to encourage people to engage in protective health behaviours in the context of adverse weather events. This refers to both what is communicated and how it is communicated.
We address three questions:
- What UK and international evidence currently exists on the effectiveness of public health messages disseminated for adverse weather events, for general and at-risk populations?
- Which communication channels used for adverse weather events (for general and at-risk populations) are most effective and why?
- What factors influence the public’s risk perception and health and wellbeing behavioural responses in relation to adverse weather events?
We begin with a summary of evidence on the effectiveness of public health communication (RQ1, Chapter 4), before turning to an examination of the factors shaping risk perception and behaviour (RQ3, Chapter 5). Understanding these factors provides the context to interpret communication effectiveness and informs the implications for communication (Chapter 6). We turn to evidence on communication channels (RQ2, Chapter 7), before situating the findings within the wider evidence on public health and disaster risk communication (Chapter 8) and drawing together overall conclusions and directions for future research (Chapter 9).
Methodology
The research involved two interlinked phases. In Phase 1 we carried out a desk-based literature review, implemented as a Rapid Evidence Review (RER). In Phase 2 we conducted a series of interactive workshops and interviews with organisations representing at risk groups, to further explore people’s responses to adverse weather health messaging. The design and implementation of both phases were developed in consultation with the project’s Steering Group and agreed at key decision points throughout.
Full methodological details are in Appendix A. Some related issues are outside the scope of this research. These are set out in Section 12.4.
RER findings and nature of the evidence base
Weather event and geographic coverage
We included 32 studies (26 peer-reviewed articles and 6 grey literature items). Most focussed on heat (n = 20). A comparatively smaller number addressed drought (n = 4), floods (n = 2), cold and heat (n=2) and multiple hazards (n = 4). The latter included floods and, to a lesser degree, heat (alongside other extreme weather events that were out of scope). Cold weather as a standalone weather event was not represented. Nine studies were UK-based, alongside those from the USA (n = 5), Canada (n = 4), and Australia (n = 2). The evidence reviews in the sample (11) drew on a wider international evidence base, encompassing countries within the target range as well as others in Asia, and South America. Most studies addressed more than one research question.
The heat literature is the highest in volume and the most varied. Heat is also the weather event with the strongest evidence of effectiveness. The following table provides an overall summary of the studies included in this RER.
Study type | Nature of evidence and number of studies | Reference and detail on approach | |
|---|---|---|---|
Heat RQ1 | Intervention studies (n=3) Test the link between a targeted communication intervention and changes in knowledge, behaviour, and/or health outcomes. | All focus on vulnerable groups and use RCTs (n=2) or quasi-experimental designs (n=1). |
|
Heat RQ1 RQ2 RQ3 | ‘Real world’ exposure studies (n=4) Public responses to heat-health messaging delivered through campaigns or during heat events. | Analysis of a nationally representative survey in England (n=1); non-representative surveys in the UK and Australia (n=2); mixed methods evaluation (n=1). Provide evidence on information reach, and factors mediating the relationship between information exposure and behavioural response. |
|
Heat RQ1 RQ3 | Message experiments (n=2) Experimental designs to test the impact of particular framings on behavioural intentions, allowing controlled testing of factors that influence perceptions and behaviours. | Tested the influence of messages that recall negative heat experiences (n=1). Tested the influence of perceived message relevance (n=1). Their results provide insights into message design. |
|
Heat RQ1 RQ2 RQ3 | Other empirical/practice-based guide (n=6) Examine communication practices for factors influencing behaviour, barriers, facilitators, and insights on improving content, reach, or channels. | Content analyses of social media (n=2) and public authority websites (n=1); expert consultation on warning message content (n=1); qualitative study exploring barriers to, and opportunities for improving, communication effectiveness and reach (n=1); good practice toolkit (n=1) |
|
Heat RQ1 RQ2 RQ3 | Determinants of perception and behaviour (n=5) Survey, reviews and empirical studies. | Nationally representative risk perception survey (n=1); survey testing the influence of personal experience of heat symptoms and risk perception on protective behaviour (n=1); evidence reviews on behaviours taken during heat events and/or determinants of heat-health behaviour (n=3). They include Implications for message design and/or channels. |
|
Heat/cold RQ1 RQ3 | Factors affecting health/risk perception (n=2) Survey and scoping review | Nationally representative survey (n=1); scoping review (n=1). Focus on older adults and draw out implications for message content. |
|
Floods RQ1 RQ2 RQ3 | Evidence reviews (n=2) (communication effectiveness) | Systematic review on barriers to flood risk communication (n=1) and rapid evidence assessment with stakeholder interviews and workshops (n=1) Examine how information is communicated, what influences perceptions of flood risk and behavioural responses and implications for content/channels. |
|
Mixed hazards (floods and heat) RQ1 RQ2 RQ3 | Evidence reviews (n=4) (communication effectiveness; determinants of behaviour) | Components or evidence of communication effectiveness (n=3), and motivational factors that influence behavioural responses (n=1). All included floods, and one included floods and heat (alongside hazards out of scope). |
|
Drought RQ1 RQ2 RQ3 | Mixed approaches and evidence (n=4) | Content analysis of social media and media coverage (n=1), examining what is being communicated and how; participatory study (n=1) exploring the challenges of communicating drought risk with findings relevant to message design and channels; systematic literature review of factors influencing drought vulnerability and resilience (n=1); guidance document (n=1). |
|
Limitations of the evidence base
The evidence base linking adverse weather messaging to behaviour or health outcomes (RQ1) is limited. Where it does exist, it is concentrated in the heat literature. No studies test the effectiveness of different channels. This means that RQ2 on the effectiveness of communication channels is the least well-evidenced. By contrast, the literature on all four weather events provides stronger insight into the mechanisms that shape communication outcomes (RQ3). This includes evidence on how people perceive and interpret risk, what influences protective behaviour, the barriers that constrain action, and the factors that affect whether communication is acted upon. Overall, the evidence base is therefore stronger in explaining the conditions under which communication is more or less likely to succeed than in identifying which specific messages or channels are most effective.
Some studies fall outside a public health frame. For instance, flooding has been extensively examined in the risk and emergency response literature, focusing on property protection, evacuation, and early warning systems, rather than on public health behaviours such as coping with psychological distress. Similarly, some of the heat literature focuses more broadly on weather warnings and risk communication than specifically on public health messaging, and evidence on drought mainly addresses water conservation rather than wider health-focused messaging. Insights from these studies are applicable to our research, but demonstrate the limited research available on broader public health messaging. Much of the available evidence focuses on the response and preparedness phase of the disaster management cycle, with limited attention to the recovery phase or to how communication can support longer-term behaviours and resilience.
Experimental studies used in our review cite limitations related to generalisability, such as limited randomisation, dropout rates, study timing, or response accuracy (e.g., self-reported changes in health). Broader empirical research also faces sampling limitations, including uneven geographic coverage, potential exclusion of some groups, and non-representative samples, all of which affect generalisability. Reliance on self-reported changes in behaviour and retrospective recall may further reduce accuracy in these studies.
Limitations of our approach
While the RER approach balances rigour and efficiency, it is more limited in scope than a full systematic review. Selection decisions considered both the quality of evidence and its relevance to the Scottish context. Non-English-language literature was excluded. Therefore, relevant international evidence may not have been captured.
Our search included grey literature, but we prioritised sources that evaluated communication activity, were explicitly evidence-based or where they supplemented limited peer-reviewed evidence (e.g. drought). Some practice-based insights may be missed.
Phase 2 balanced breadth of insight with the constraints of a time-limited study. It included engagement with national and local organisations, and two place-based community workshops. While these provided valuable lived-experience insights, they reflect the views of a relatively small number of participants.
Evidence on effectiveness of public health messages disseminated for adverse weather events
This chapter summarises evidence on the effectiveness of public health communication. Ultimately, public health communication aims to reduce morbidity and mortality resulting from an adverse weather event (Health Canada, 2020). However, none of the items included in this review directly investigate the link between public health communication and mortality, and only a few make the link between communication and health outcomes (including health services use). Most focus on linking public health communication to what Health Canada (2020) calls intermediate steps towards reduced morbidity and mortality: raising awareness, increasing knowledge, changes in health-related behaviour (or intended behaviour change), developing skills for behaviour change. We present evidence around these outcomes in the next sections.
In 4.1 we present findings from the three studies that evaluated targeted communication interventions. All three identified changes in behaviours, and two identified changes in health outcomes. In 4.2 we synthesise the evidence from four studies that examined associations between exposure to general heat-health messaging and self-reported awareness, recall, and behaviour change (or intentions) in real-world settings. Findings across these studies suggest a more uneven pattern: heat-health messages can be associated with increased awareness and reported protective action for some groups, but effects can be modest and do not reliably extend to those most at risk.
Evidence from targeted intervention studies
Robust evaluations using experimental designs to assess the effectiveness of public health communication on behaviour change are comparatively rare. Three such studies, all related to heat (Mehiriz, 2018; Nitschike et al., 2017; Takahashi, 2015), evaluated the impact of specifically designed communication interventions on health protective behaviour during heat waves on vulnerable people in Canada, Australia and Japan respectively. The two studies using RCTs also examined impact on health outcomes (Mehiriz et al, 2018; Nitschike et al., 2017), and the study using the quasi-experimental design measured changes in knowledge of heat-adaptive behaviours (Takahashi, 2015).
Four key findings emerge. First, all three studies showed a statistically significant difference in health protective behaviour between treatment and control groups. Those receiving ‘treatment’ in the form of health advice (e.g. via warnings, information packages or automated phone warnings) were more likely than those not receiving those messages to adopt protective behaviour.
The sub-set of two studies using RCT designs found a link between changed behaviour and health outcomes. Nitschike et al.’s (2017) RCT of an information package for older people in Southern Australia during a heatwave found that the intervention was associated with a significant reduction in heat stress, indicating a measurable health outcome linked to the behaviour change. An RCT evaluating the impact of an automated telephone message warning vulnerable people of heat episodes and providing recommendations about protecting their health in such circumstances (Mehiriz et al., 2018) identified a reduction in health service use among a sub-group of message recipients (women and particularly women with chronic illnesses). The treatment group adopted more of the recommended behaviours than the control group, though the study did not find a reduction in heat related illnesses.
Second, the quasi-experimental study by Takahashi et al. (2015) suggests that behaviour change effects of public health communication can be enhanced with reinforcing interventions. They found that supplementing the heat health warning with receipt of bottled water led to the adoption of additional protective behaviours and better performance regarding frequency of water intake and cooling the body compared to the control group that only received the heat health warning. Importantly, these behaviour changes occurred in the absence of increases in knowledge and awareness of how to prevent heat related illness. The authors suggest that the physical presence of the water bottle functioned as both a prompt and an enabler, acting as a visible reminder of exactly what to do.
This leads to a third finding from this study: improvements in knowledge and awareness are not preconditions for behaviour change.
Fourth and finally, Meheriz et al. (2018) suggest that paying attention to intersections when analysing the results of heat messaging interventions (and, arguably, designing messages) is important, as these interventions may benefit different subgroups differently.
Evidence from ‘real world’ campaigns
Four studies in our corpus examine public responses to general heat-health messaging delivered through campaigns and alerts in ‘real-world’ settings (Erens et al., 2021; Lefevre et al., 2015; Oakman et al., 2010; Williams et al., 2019). These real-world exposure studies investigate whether people recall hearing health protective advice and whether they report changing their behaviour as a result.
Across these studies, the relationship between exposure to advice and self-reported behaviour change is not consistent. Hearing public health information is associated with stronger intentions to act for some individuals, but effects can be modest and uneven. In a UK-wide survey conducted in October 2013 to examine public responses to heat protection messages during the 2013 England heat wave, Lefevre et al. (2015) found a positive link between hearing heat-protection recommendations and intentions to implement them. Oakman et al.’s (2010) evaluation of the Beat the Heat: Don’t forget your Drink Campaign in Australia and Williams et al.’s (2019) survey of knowledge, attitudes and behaviour of the general population during the 2017 heatwave in England show a modest effect on self-reported behaviour change: 54% and 42.9% respectively of people hearing heat health advice reported changing their behaviour as a result.
The studies also indicate that behavioural responses vary across population groups. Women (Oakman et al., 2010), people with limiting long-standing illnesses (LLSI) (Williams et al., 2019), and younger people (Lefevre et al., 2015) were more likely to adopt protective behaviour. Erens et al. (2021) found that fewer than one third (26.8%) of older people (75 years and over) and just over a quarter (25.6%) of adults in poor health reported changing their behaviour after hearing heat-health advice issued during the 2013 England heat wave. This suggests that some population groups potentially at risk are not very likely to take protective action.
This lag between message exposure and behaviour change is also supported by the wider literature on determinants of risk perception and behaviour. In the heat literature, nationally representative survey evidence (British Red Cross, 2023), systematic and narrative reviews of heat-protective behaviours and behavioural determinants (McLoughlin et al., 2023; Vu et al., 2019), and several empirical studies (Li and Howe et al., 2023; Olson et al., 2023; VanderMolen et al., 2022) collectively point to a gap between awareness of risk and the uptake of protective action. The same observations emerge from literature on floods (Henderson et al. 2022) and drought (McClymont et al. 2022). Together, this body of evidence shows that there is no linear relationship between awareness and knowledge of the health risk associated with an extreme weather event and taking protective action.
Summary
The three intervention studies show that public health communication can encourage behaviour change with consequences for health and health service use. Individual studies further suggest that these outcomes can be enhanced by providing supplementary interventions (such as water delivery) and can differ by population group. Evidence from real-world campaigns, however, paints a more complex picture. It shows that providing information can encourage some people to change behaviour. However, some of those most likely in need of protection are less likely to do so.
The role of risk perception
Risk perception refers to how individuals assess both the likelihood of a hazard and their own susceptibility to its consequences. This is described as part of a ‘threat appraisal’ process, which includes both perceived risk (how likely the threat is) and perceived vulnerability or susceptibility (how likely it is to affect them) (McLoughlin et al., 2023; Olson et al., 2023). These factors are important predictors of protective action: individuals who perceive themselves as personally at risk from health-related threats are more likely to adopt protective or adaptive behaviours (Henderson et al., 2022; McLoughlin et al., 2023).
Given the maturity of the literature on factors influencing risk perception and behaviour, our evidence search for this research question was designed to prioritise the strongest available evidence, particularly evidence reviews. As a result, this chapter draws on 11 evidence reviews examining risk perception, behavioural determinants, and factors affecting effective communication across heat (n=3), heat and cold (n=1), drought (n=1), mixed hazards (n=4), and flooding (n=2). However, evidence relevant to this question was discussed across a broader proportion of the included literature. The review evidence is therefore supplemented by empirical and practice-based literature which includes studies directly examining: factors affecting risk perception and protective behaviour across heat (n=8) and heat and cold (n=1); and communication practices and message content through a behaviour change lens across heat (n=5) and drought (n=2). These are further supplemented by two practice-based communication toolkits focused on heat and drought communication.
This chapter presents findings from included studies, focusing on: knowledge and awareness (section 5.1), the role of experience and proximity to an extreme weather event (section 5.2), efficacy (Section 5.3), the role of emotions (Section 5.4) as well as temporal and spatial issues (Section 5.5), socio-demographic and socio-economic factors (section 5.6) and the role of social norms and trust (section 5.7). Woven into this narrative are findings from our stakeholder engagement to illustrate points made in the literature.
Knowledge and awareness
Although providing information can have a positive effect, the reach of these communications is uneven. Erens et al. (2021) found that only just over half of respondents (51.0%) reported being aware of hot-weather-related health publicity or advice during this event. This increased to about two-thirds (63.9%) of respondents who were vulnerable. Williams et al (2019) found older people aged 75 and over, as well as residents of warmer regions like the Southeast of England, were more receptive to hearing health protection messages, as are households with children (Williams et al., 2019) and women (Oakman et al., 2010). Evidence from multiple weather events and drought further suggests that groups on low income and digitally excluded (Coombs et al., 2024; McClymont et al., 2022) appear to be less likely to access or hear advice. These studies show that already at the first step (accessing or hearing messages) public health messages can fall short in reaching a substantial portion of audiences.
Beyond this, hearing or being aware of messages does not necessarily translate into understanding, retaining or absorbing the information conveyed (British Red Cross, 2023; Erens et al, 2021; Henderson et al, 2022; Olson et al, 2023; Ratwatte et al, 2022; McIntyre et al, 2019; VanderMolen et al, 2022; Vue et al, 2019). The 2023 British Red Cross survey found that those most at risk from heat – including pregnant women and those with a child under three (29%); people who work outdoors (62%), and those with a heart condition (57%) – did not know how to protect themselves.
But even among those who are well informed, many do not take action. Erens et al. (2021) report that people had only partial knowledge of heat-protective actions after hearing the 2017 heat-health advice. Vulnerable people have been shown to be affected because of challenges with complex language, information overload and contradictory information (McIntyre et al, 2019). Older people can suffer from poor message recall and a lack of understanding of what to do (Vu et al., 2019). This was also highlighted in our engagement activities.
Our stakeholder engagement with Scottish organisations representing ethnic minority groups and Gypsy Traveller communities found that literacy barriers can be a challenge to understanding public health messaging. In the case of ethnic minority groups, some may not understand English or understand new weather concepts. If members of Gypsy Traveller communities experience literacy challenges, they tend to navigate digital devices using visual cues (such as remembering app icons) and peer to peer learning. Scottish organisations working with people from warmer climates and for whom English is not their first language said that concepts such as “cold water shock” may be completely unfamiliar.
There is thus no linear relationship between risk communication and behaviour change (Olsen et al, 2023; VanderMolen, 2022; Henderson et al, 2022). Indeed, the wider literature on heat (British Red Cross, 2023; Li and Howe, 2023; McLoughlin et al., 2023; Olson et al., 2023; Tan et al, 2024; Takahashi et al, 2015; VanderMolen et al., 2022; Vue et al., 2019) and flooding (Henderson et al, 2022) suggests that there is no direct causal link between awareness and knowledge of the health risk associated with an extreme weather event and taking protective action.
Experience of adverse weather
Direct, tangible experiences can shape perceptions and actions, often more powerfully than information alone.
Studies on heat show that negative health-related episodes (such as illness, exhaustion, or severe discomfort) are more influential than simple exposure to high temperatures (Bruine de Bruin et al., 2016; Esplin et al., 2019; Lefevre et al., 2015; McLoughlin et al., 2023; Williams et al., 2019). These encounters make risk feel concrete and increase receptivity to guidance and intentions to act. Although the evidence base for cold is smaller, it shows a similar pattern: Ratwatte et al. (2022) report that older adults who had not recently experienced illness during extreme temperatures tended to downplay their vulnerability.
Drought appears to have a distinct challenge: absence of experience leads to a lack of interest in the topic in places like Scotland and Ireland (Antwi et al, 2022). The lack of personal and collective memory of drought in the UK make it harder for people to draw on lived experience when interpreting risk (Weitkamp et al., 2020). Moreover, “drought issues are much less personal unless people are directly affected, such as no water coming out of the tap” (Global Water Partnership, 2019 p. 20). This lack of experiential reference points weakens drought risk perception and limits the ability of communicators to activate the ‘availability heuristic’- the cognitive process through which people judge risks based on how easily relevant examples come to mind. However, where drought experience does exist, for example in regions reliant on private water supplies (e.g. rural communities), it can heighten awareness, perception, and preparedness (McClymont et al., 2022), which also illustrates how spatial context acts as an intervening factor.
Our place-based engagement work with Dumfries and Galloway highlighted that while many local residents understand flood dynamics and take precautions like checking river levels themselves, tourists and new residents often fail to heed warnings, due to lack of experience or underestimating the risk. Residents we spoke to described people not from the area driving through flooded roads despite clear signage, leading to hazardous situations.
Experience therefore functions as a form of evidence, ‘anchoring’ risks in memory, shifting them from abstract to tangible, and heightening perceived personal susceptibility. This explains why several studies suggest using communications that prompt recall of negative or uncomfortable prior experiences to strengthen engagement (Bruine de Bruin et al., 2016; Esplin et al., 2019; Lefevre et al., 2015; Li et al., 2018; McLoughlin et al., 2023).
Efficacy as a bridge to action
However, recognising a threat is not always enough. A well-documented phenomenon, often referred to as the “risk perception paradox” (Wachinger et al., 2013), shows that people can be aware of a threat and acknowledge personal vulnerability, yet still fail to take protective action. Protection Motivation Theory (PMT) (Forsyth et al., 2023; Henderson et al., 2022; Tan et al., 2024) is one framework that clarifies the process of ‘conversion’ from perceiving a risk to being motivated to act. It suggests that protective action depends not only on perceiving a risk (threat appraisal) but also on ‘coping appraisals’ (McLoughlin et al., 2023), which include believing that the recommended protective actions are effective (response efficacy) and achievable (self-efficacy), and that the costs of those measures are affordable.
These beliefs consistently emerge among the strongest predictors of adaptive behaviour, surpassing knowledge-based determinants and demographic factors (Bourret Soto et al., 2024; British Red Cross, 2023; Erens et al, 2021; Forsyth et al., 2023; Henderson et al., 2022; Lefevre et al, 2015; McIntyre et al., 2022; McLoughlin et al., 2023; Ratwatte et al., 2022; Tan et al., 2022; Turner et al., 2024). Tan et al. (2022) found that self-efficacy, response efficacy, and personal attitudes exerted the strongest influence on protective behaviours across disaster types, a finding supported by McIntyre et al. (2022). The importance of efficacy beliefs also emerges in evidence reviews across heat (Bourret Soto et al., 2024; McLoughlin et al., 2023), floods (Forsyth et al., 2023; Henderson et al., 2022), and heat and cold (Ratwatte et al., 2022).
UK-based empirical studies on heat also support these findings (British Red Cross, 2023; Erens et al, 2021; Lefevre et al, 2015), with both Lefevre et al. (2015) and Erens et al. (2021) showing that perceived effectiveness of recommended behaviours was a strong determinant of, respectively, intention to act or self-reported behaviour change during heat events. Erens et al. (2021) further found that different socio-demographic groups perceive different recommended protective measures as highly effective. Adults potentially vulnerable to heat because of chronic conditions showed the lowest confidence in the effectiveness of most recommended behaviours compared to the other groups.
Even when a behaviour is perceived as effective, people may not act on it. For example, practical reasons can get in the way, inhibiting adoption of risk-mitigating behaviours. These can include one’s capability to act (e.g., physical mobility, literacy), opportunities and access to interventions (e.g., vehicle to drive to cooling centre, financial resources to invest in or run air conditioning or safety concerns (e.g. when opening windows).
These findings are consistent in several studies on heat (British Red Cross, 2023; Erens et al., 2021; Esplin et al., 2019; Olson et al., 2023; Heat Health Canada, 2020; Vu et al., 2019; Tetzlaff et al., 2025b), and extend to heat/cold (Turner et al., 2024), floods (Henderson et al., 2022) and drought (McClymont et al., 2022) which also suggest that individuals balance awareness and intent against the financial, physical, and practical realities of implementation.
During our engagement events with Scottish organisations working with parents and carers of infants and young children, participants shared that single parents face logistical challenges, such as finding childcare to leave the house, for necessary preparations such as topping up pay-as-you-go electricity meters. Keeping warm in cold weather is expensive, especially in energy-inefficient housing; running fans or stalling air conditioning for rising temperatures also poses a cost barrier for low-income families. Cultural factors can shape propensity to act. Organisations working with diverse communities mentioned that strict cultural gender roles, e.g. in the Gypsy Traveller community, can mean women may not take actions deemed to be ‘men’s work’.
Perceived control, or the belief that actions can make a difference, also matters. Studies on floods (Henderson et al., 2022), heat (McLoughlin et al., 2023), and heat and cold (Ratawatte et al., 2022; Turner et al., 2024) suggest that stoicism or fatalism (‘putting up with it’) can reduce motivation by viewing weather as something to ‘endure’ rather than manage. This reflects an external locus of control, where events are seen as governed by fate or nature, lowering the perceived value of action. While the relationship between perceived control and behaviour is mixed, Ratawatte et al. (2022) found one study which showed that reframing messages to emphasise individual agency, i.e. supporting an ‘internal locus of control’, increased perceived risk and adaptive intentions.
During our engagement events organisations working with diverse communities mentioned the faith-based culture of the Gypsy Traveller community, with its deep belief in omens and signs. This can lead members to prioritise faith over taking immediate, practical safety measures.
Esplin et al. (2019) and Henderson et al. (2022) further highlight that motivation can be undermined by a limited sense of personal responsibility, whereby individuals shift responsibility onto others (e.g. governments) and therefore do not act.
The role of emotions
Discomfort, fear and concern can mediate the relationship between heat exposure and protective intentions. Yet in the UK, while concern about hot summers is rising (British Red Cross, 2023; McLoughlin et al., 2023), positive associations with warm weather are still prevalent and dilute these effects (Bruine de Bruin et al., 2016; Erens, 2021; Lefevre et al., 2015; Turner et al., 2024; Weitkamp et al., 2020; Williams et al., 2019).
Analysing responses to the 2013 UK heatwave, Lefevre et al. (2015) found that while heat-protection messages appeared to strengthen beliefs that recommended actions would be effective, they were also associated with more positive emotions about heat, which in turn reduced uptake of protective behaviours. The authors argue that, in the UK context, warnings about hot weather may inadvertently trigger positive memories and emotions associated with summer, thereby weakening the perceived need for protective action. Bruine de Bruin et al. (2016) tested whether recalling past unpleasant temperatures was linked to intention to take up health protective behaviours. Their UK-based experimental study on messaging strategies found that asking people to recall the “most unpleasant highest temperature” successfully triggered memories of unpleasantly hot weather and increased intentions to engage in heat-protection behaviours. By contrast, asking participants to merely recall the highest temperature led to pleasant memories of warm weather, reducing motivation for protection; asking participants to recall the most unpleasant temperature in the summer typically led them to recall cold (summer) weather, which did not encourage heat protection.
Our stakeholder engagement workshops illustrated how negative experiences with cold can lead to fear and impact on individuals’ capacity to access help. One workshop participant shared the experience of a friend being very scared of going out after falling during cold, slippery weather two years prior. Another participant recalled a personal and scary experience of falling while pregnant and walking to the GP in bad weather, highlighting the difficulty of accessing essential services like GPs during extreme weather, especially when a person is vulnerable. In the Gypsy Traveller community, older generations can interpret messages very literally, leading to extreme fear from generalised news warnings.
Drought inherits similar emotional biases. Dry weather in the UK is often viewed positively because it typically co-occurs with sunshine. Weitkamp et al. (2020) describe an informal ‘weather hierarchy’ in which sunny, dry days are valued over cool, wet ones, making it difficult to frame drought as a risk. In the case of flooding, fear can prompt defensive coping (denial, fatalism, or disengagement) unless people know how to protect themselves (Forsyth, 2022). Similarly, Tan et al. (2022), covering multiple hazards (including flooding), found that negative affect (fear, worry, anxiety) had only a moderate effect on protective behaviour, compared with response and self-efficacy. Bruine de Bruin et al. (2016) reinforce this point, noting that emotion-based strategies may still fail if people do not understand why or how a behaviour is effective.
Temporality and spatiality
Temporality and spatiality shape experiential and emotional processes. Temporal context involves timing and sequence of experience and communication: how proximity in time and recent weather influence perceptions of risk as urgent or remote, credible or irrelevant. Bruine de Bruin et al. (2016) found that a message sent three months after a heatwave during cooler weather made people recall ‘highest temperatures’ as pleasant, reducing protective intent. When messages were sent during hot spells, people recalling ‘unpleasant temperature’ were more likely to remember hot days as unpleasant. The positive feelings associated with hot weather were weaker, making heat seem more unpleasant. Therefore, recent, vivid discomfort increases perceived relevance, while memories soften or become more positive over time, especially after cooler weather.
For drought, temporality operates differently. Its slow onset nature can create ‘temporal invisibility’, making it difficult for people to recognise it as a developing or personal risk (Weitkamp et al., 2020). In addition, if rainfall coincides with official drought messages, people may struggle to reconcile those messages with the immediate experience of rain (e.g., McClymont et al., 2022). Although the literature on drought focuses on water use and warning systems (outside the scope of this RER), its broader relevance lies in further illustrating how factors such as timing, sequencing, and contextual alignment can shape whether communication is perceived as credible, plausible, and personally relevant.
Spatial context includes geographical location and living environments, influencing exposure and proximity to weather. Urban areas experience stronger heat-island effects, which increase awareness (Health Canada, 2020; Tetzlaff et al., 2025a). Housing conditions such as top-floor flats or poor insulation increase exposure to heat or cold. Older adults in southern England see themselves as less at risk from heat than those in the Midlands or North, despite higher temperatures, likely due to climatic normalisation or coping routines (Turner et al., 2024). Residents in Scotland and Northern Ireland, where temperatures are cooler, are less likely to take heat-protective actions, indicating lower perceived relevance (McLoughlin et al., 2023). For drought, rural households face water scarcity directly and are more prepared (McClymont et al., 2022), while most UK residents find drought abstract (Weitkamp et al., 2020).
Socio-demographic and socio-economic factors
Public health communication on adverse weather events is often particularly concerned with protecting socio-demographic groups considered vulnerable. Its effectiveness therefore relies on these demographics recognising their vulnerability and taking the recommended protective action.
However, the evidence from this RER shows that socio-demographic and socio-economic factors alone do not reliably predict how people perceive weather-related health risks or their behavioural responses, as these factors interact with psychological and contextual mediators. For instance, people living in poorer neighbourhoods and minoritised groups often report higher heat-risk perceptions, reflecting heightened exposure (McLoughlin et al., 2023). Yet responses are shaped by personal characteristics and systemic inequalities such as cost, housing conditions, physical capacity, digital access, literacy and language -factors that influence whether people receive, interpret and feel able to act on advice (linked to self-efficacy). For example, Tuner et al. (2024) found that risk perceptions of cold weather varied by socio-economic characteristics, likely indicating that those with more resources are better able to implement health-adaptive behaviours (e.g., keeping homes warm).
Age, too, does not determine behaviour. Evidence on heat and cold shows that older adults do not necessarily identify themselves as at risk (British Red Cross, 2023; Esplin et al, 2019; Li et al., 2018; Li et al., 2023; Olson et al., 2023; Ratawatte et al., 2022; Turner et al., 2024; VanderMolen et al., 2022; Vu et al. 2019; Williams et al., 2019). For example, Vu et al.’s (2019) systematic review of literature on heat health prevention measures and adaptation in older populations showed that many older people surveyed in Australia, UK, and USA/Canada did not feel they were susceptible to heat-related illness and did not feel they should stop daily activities. Williams et al. (2019), who also examined older people and those with limiting long-standing illness (LLSI), found that most participants in those categories did not consider their health to be at risk during hot weather. However, they were more likely to identify risk in others. This aligns with findings from Li et al. (2023) and Esplin et al. (2019) that individuals may accept group-level risks but exclude themselves due to active self-identification as healthy or capable. Moreover, age-related factors such as forgetfulness, reduced message recall, and absence of prompts, particularly for those living alone, still shape how older adults engage with advice (Erens et al., 2015; Vu et al., 2019). This again indicates that what matters is not age itself but how individuals interpret their vulnerability and capability, suggesting that communication strategies should take such considerations into account.
The same holds for health status. For heat and cold, Turner et al. (2024) and Ratawatte et al. (2022) found that individuals who are health-conscious, managing chronic illness or had comorbidities were more likely to engage in protective behaviours. Specifically related to heat, Lefevre et al. (2015) and Erens (2019) found that being older, female, and prone to adverse effects or poorer self-reported health were associated with greater adoption of certain protective behaviours. Again however, perceived effectiveness of an action emerged as a stronger predictor of uptake, overriding the effects health status (and age) alone.
Data on gender are consistent: women report higher risk perception, message recall and concern, and are more likely to modify their behaviour (e.g. Bourret Soto et al., 2024; Henderson et al., 2022; Mehiriz et al., 2018; Oakman et al., 2010). Despite this significance, other factors intersect, such as beliefs about the effectiveness of recommended behaviours (Bourret Soto et al., 2024; Esplin et al., 2019; Lefevre et al., 2015; McLoughlin et al., 2023; Tan et al., 2024; Williams et al., 2019). The recurrent pattern of lower perceived risk among men has led one study to explicitly suggest an engagement gap that may merit targeted communication approaches (Bourret Soto et al., 2024). This phenomenon was also highlighted by Scottish organisations involved in our stakeholder engagement, who observed the same pattern among other population groups.
A Scottish youth organisation said that boys and young men aged 12-25, particularly those not attending school, are quite vulnerable to heat as they tend to gather in parks and on beaches without proper sun protection or awareness of dehydration. Yet, they do not view heat and associated health risks such as sunburn as a significant threat and often ignore sun safety advice. And Scottish organisations representing diverse communities thought that climate migrants might underestimate their risk as Scottish weather is more temperate than that in their home countries. This might translate into a false sense of security. One workshop participant shared a personal experience of feeling dizzy and becoming dehydrated in the Scottish heat, noting it’s a different heat than she had previously experienced, and it can be dangerous.
Social norms and trust
Social influence, expressed through norms and interpersonal interactions, can play a role in shaping adaptive behaviour. Cues to action from trusted community figures and peers can help normalise protective action by making adaptive behaviours appear both common and socially approved. These dynamics operate through descriptive norms (what others typically do) and injunctive norms (what others believe one ought to do), both of which have been shown to influence intentions and behaviour in the context of adverse weather (Forsyth et al., 2023; McLoughlin et al., 2023; Tan et al., 2024). Such cues carry both descriptive and injunctive weight: they show that protective behaviours are socially visible and socially endorsed. McLoughlin et al. (2023) also note that some studies have found that their effect is strongest when individuals feel they have perceived control, showing how coping appraisals remain relevant as well.
Prosocial norms add another layer, although the evidence is weaker. One study (Esplin et al., 2019) shows that norms grounded in altruism, care and reciprocity, such as encouraging people to “check on neighbours”, can motivate behaviour. The study did find age differences in this regard, with older adults often expressing altruistic motivations, acting to safeguard others’ wellbeing, whereas younger adults focusing more on self-protection. The authors concluded that tailoring communication to these orientations could strengthen engagement. For example, interactions with older adults can emphasise the need to take care of one’s health so that one can help others effectively, and outreach to younger adults can encourage them to be more aware of vulnerable people around them and what they can do to help. However, because not everyone is embedded in strong social networks, messaging must avoid assuming access to family or community ties (Tetzlaff et al., 2025a).
Finally, numerous studies highlight trust as an important predictor of protective behaviour (Coombs et al., 2024; Fathollahzadeh et al., 2023; Forsyth et al., 2023; Global Water Partnership, 2019; Health Canada, 2020; Henderson et al., 2020; McIntyre et al., 2019; VanderMolen et al. 2022; Weitkamp et al., 2020). Trust in institutions, authorities and information sources affects whether public health messages are believed, prioritised or dismissed. High trust can strengthen response efficacy (confidence that guidance will help), whereas low trust can create scepticism or resistance, even when messages are well-designed. This points to the importance of considering not only message content, but also who delivers information, which will be discussed in Chapter 7.
Summary
Risk perception and behavioural responses to adverse weather emerge from the interaction of multiple influences. Socio-demographic and socio-economic characteristics shape opportunities and constraints; personal experience, proximity, emotion, and the wider spatial, temporal, and cultural contexts condition whether risks feel salient; efficacy beliefs translate risk perception into motivation; social norms, cultural identities, and trust influence whether protective behaviours are viewed as credible, relevant, and socially supported.
The evidence converges on several common themes:
Experience and emotion make risks tangible, but their influence depends on wider contextual cues and on whether individuals believe action is both possible and worthwhile.
Efficacy consistently emerges as a central mechanism linking perception with action, although it is sensitive to structural barriers.
Social and cultural environments—including prevailing norms, collective narratives about weather, and trusted relationships with messengers—shape how people interpret advice and whether they act on it.
Demographic factors amplify rather than predict behaviour, operating through intervening cognitive and contextual processes.
Taken together, the findings reinforce the value of viewing behavioural responses as the outcome of interconnected processes, shaped simultaneously by individual interpretation and the wider conditions in which people live.
Implications for public health communication
Considering this complex web of factors shaping the relationship between exposure to public health communication on adverse weather and subsequent action, the literature included in this RER, and qualitative evidence from stakeholder engagement highlight several implications for how messages should be designed to support behaviour change.
Persuasive and comprehensible messages
Olson et al. (2023) and Li et al. (2018) argue that messages need to be designed to be persuasive. This requires going beyond merely increasing understanding to include additional information intended to increase message recipients’ perceived severity of the situation and their susceptibility. For example, information about how heat will personally affect an individual can increase perceived severity, which strongly predicts the extent to which individuals adopt heat-mitigation behaviours. However, the authors’ quantitative content analyses of official heat-related tweets found that agencies underuse such message components. Although both studies focus on official agency communication during extreme heat events rather than public health messaging more broadly, they nevertheless provide transferable insights: behaviour change is more likely when messages actively engage perceptions of personal relevance and risk, rather than relying on information provision alone.
Messages must also be designed so that recipients can easily absorb their content, and audiences need to correctly understand the message (Coombs, 2024; Health Canada, 2020; McClymont et al., 2022; Olson et al., 2023; Tetzlaff et al., 2025a). According to Coombs et al.’s (2024) scoping review on factors affecting public health communication, current research highlights the importance of tailoring public health messages to specific audiences by considering language and literacy diversity, income levels, geographic differences, and health and other needs and preferences. Tetzlaff et al. (2025a) used terms such as ‘living space’ or ‘cooler area’ instead of ‘house’ or ‘basement’ when revising heat-health warning messages to reflect varied housing conditions. Similarly, Health Canada’s good practice toolkit (2020) emphasises that messages should address the audience’s abilities and unique challenges and perspectives. Practical advice from this body of literature is:
User testing of messages with diverse (including vulnerable) groups to identify misunderstandings, knowledge gaps, or ineffective phrasing (Olson et al., 2023).
Readability testing to ensure messages can be read and understood by audiences with lower health literacy, non-native speakers, or newcomers (Tetzlaff et al., 2025a).
Beyond this, McLoughlin et al. (2023) recommend practical inclusivity measures such as messages in multiple languages to reach tourists, using creative forms of communication (e.g. art, soap opera storylines, late-night radio) and designing materials that resonate with specific audiences (e.g. eye-catching leaflets, for example for older adults).
Literature across heat (Bourret Soto et al., 2024; Health Canada, 2020; Oakman et al, 2010; Olson et al., 2023; Tetzlaff et al., 2025a; VanderMolen et al., 2022), flooding (Forsyth et al., 2023; Henderson et al., 2022) and drought (McClymont et al., 2022; Weitkamp et al, 2020) further argues that messages need to include actionable guidance which explains the rationale behind protective behaviours. For example, Oakman et al.’s (2010) study of the Australian “beat the heat” campaign showed messaging suggesting concrete daily quantities for liquid intake of 1.5-2l was effective in provoking recall of the message and what to do in heat (drinking water). Tetzlaff et al.’s (2025a) review of heat warning messages with public health and climate expert input started all messages with verbs (e.g. check, drink, plan, move, monitor) to make them directive and concrete and increase their potential to encourage protective behaviours. This can be supported by including simple infographics and daily schedules (Bourret Soto et al., 2024).
A focus on action is also a key message coming out of our stakeholder engagement, especially action that is low-cost and realistic which recognises differences in financial situations. Scottish organisations argued that general advice such as putting “baby items” in grab bags for emergencies does not inspire action without specifying what these items are (like nappies and bottles).
This guidance also needs to recognise that an adverse weather event can be experienced differently across spatial contexts. For example, people in rural areas experience and respond to heat differently from those in densely populated cities. They may also have more limited access to specific resources (e.g. cool or warm places to go to) (Tetzlaff et al., 2025a). Given that certain socio-economic factors may prevent people from changing their behaviours, communication is more likely to change behaviour when complemented by programs that remove barriers to action and provide opportunities for citizens to adopt coping strategies (e.g. providing free bus tickets to people during extreme heat will encourage them to go places where they can cool down) (Health Canada, 2020). Devising these programmes is, however, out of control of public health communicators.
Beyond this, Health Canada (2020) recommends that message content be simple, specific, and motivating, and that it use plain, jargon-free language and personal pronouns (‘you’). Based on a qualitative content analysis of heat health information on public health websites, Tetzlaff. et al (2025a) argue that message content It should be evidence-based, using simple infographics, directly mentioning the most important contexts where the risk is greatest.
In our engagement with Scottish organisations representing diverse communities, they recommended the use of storytelling to deliver the message more effectively. For example, through faith-based teachings or community gatherings.
Communicating the benefits of health advice
Evidence from qualitative (VanderMolen et al., 2022) and quantitative (Li et al., 2018; Olson et al., 2023) empirical studies as well as systematic and scoping literature reviews (Bourret Soto, 2024; McLoughlin et al., 2023) focusing on heat conclude that to evoke belief in the effectiveness of a measure, public health messaging needs to go beyond describing (heat) advice to also indicate why a particular behaviour is crucial to protect oneself. This information can increase perceived response efficacy (i.e., the belief that the behaviour is effective in mitigating a threat) and self-efficacy (i.e., confidence in their ability to act). Both have a powerful effect on behaviour change. Therefore, the association between the hazard and the protective action should be included in the message (McLoughlin et al. 2023):
Prior experience: “Think back to the last time you felt overwhelmed by the heat, perhaps sick or faint with heat stress. This is the reality of heat risks consequences.”
Addressing positive affect: “While in the past we may have looked at summer heatwaves as reasons to feel positive, we must now view such events with concern. Heat risks can lead to death and lasting health consequences.”
While emotions influence perceptions and behaviours, evidence across hazards remains mixed regarding its effectiveness as a behaviour change tool on its own. What emerges consistently, is that emotional or experiential cues alone are insufficient unless combined with efficacy information. McLoughlin (2023) emphasises that while fear or concern can heighten responsiveness, they are effective only when accompanied by clear, actionable guidance. Evidence from flood-preparedness research mirrors this finding: Forsyth (2022) shows that messages inducing fear without efficacy prompts often lead to defensive coping, such as denial, fatalism, or disengagement, whereas those combining fear with practical steps encourage problem-focused coping. Similarly, Tan et al. (2022) found across multiple natural hazards (including flooding) that negative affect (fear, worry, anxiety) had only a moderate effect on protective behaviour compared with response and self-efficacy. They caution that relying on fear alone is unlikely to produce sustainable changes in behaviour.
Maintaining personal relevance
As people do not like to think of themselves as vulnerable, messaging that uses vulnerability labels may reduce personal relevance and weaken engagement (Erens et al., 2021; Ratawatte et al., 2022; Turner et al., 2024). “Public health messages should avoid labelling individuals as ‘vulnerable’ when raising awareness of the risks of hot weather, even among those who fit the definition” (Erens, 2021). Evidence from a systematic review on heat (Bourret Soto et al., 2024) and an RCT on heat risk messaging (Li et al., 2023) show that designing messages to emphasise “everyone can be at risk” can be effective instead.
Li and Howe (2023) examine this in depth, specifically testing different framings in heat-risk messages targeted to the general public. The study is informed by the broader body of research suggesting that underestimation of personal risk, i.e. low ‘perceived susceptibility’ or lack of ‘personalisation’, is a key psychological barrier to taking protective action during extreme heat events. They compared four versions of a public-facing heat risk message that varied in how they depicted which types of people were susceptible to heat-health impacts. They included: subgroup-only framing (mentioning older adults, children, people with chronic diseases, and outdoor workers); universal “everyone can be at risk” framing (illustrated in Figure 2); a combination of both; and a neutral framing. Outcomes measured included perceived message relevance, belief in hazard occurrence, perceived susceptibility, and behavioural intention.
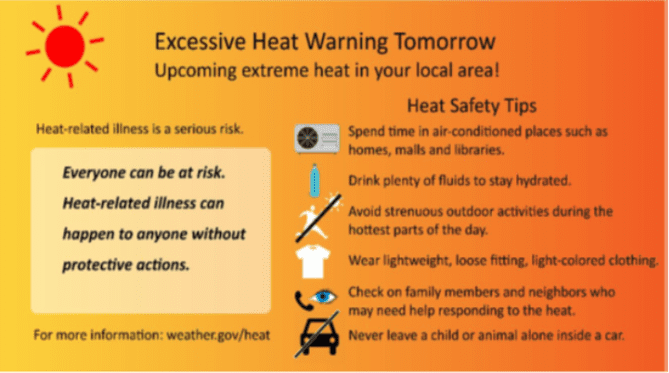
Figure 2: “Everyone can be at risk” message example (Source: Li et al., 2023)
Universal ‘everyone can be at risk’ framing produced significantly higher perceived personal relevance than subgroup listing, which scored lower on relevance even than a neutral version with no susceptibility information at all, suggesting that listing vulnerable groups in a message targeted to the general public can actively work against engagement among those who do not identify with them. This is particularly relevant given evidence suggesting that many older adults, for example, do not perceive themselves as personally vulnerable to heat, while younger people may interpret subgroup-focused warnings as implying that the threat applies mainly to others rather than to themselves. While this study is about large-scale communications that need to appeal to everyone rather than routine public health messaging, the underlying principle is transferable: how susceptibility is depicted in public-facing communications affects whether people feel the message is personally meant for them.
At the same time, improved relevance did not translate into higher perceived susceptibility or greater intention to take protective action, indicating that while relevance is a crucial first step for ‘attention’ and engagement with the message, it is not sufficient on its own to drive behaviour change. In addition, the study also found some differences: younger adults were more responsive to universal framing, while adults aged 30-44 responded more to combined ‘anyone plus subgroup’ wording. A related finding is that adding subgroup labels to universal framing weakened some of the benefits of the universal approach and, in some cases, reduced belief that the heat event would actually occur, suggesting that this may be because combining both framings sends mixed signals about who the warning is primarily intended for, potentially undermining both personal relevance and message credibility.
These findings together highlight the need to balance personal relevance, message clarity, and audience diversity in the design of heat-risk communication. They also suggest that no single framing approach is likely to work equally well across all population groups, meaning that more segmented or tailored approaches may still be needed to communicate heightened susceptibility in ways that feel personally relevant and meaningful to different audiences.
In our stakeholder engagement events, organisations representing older adults and those with chronic health conditions advised that emphasising empowerment and action rather than labelling the recipients as “vulnerable”. Being labelled as vulnerable can be a turn-off and negatively affect the message’s reception. Empowering messaging through language is more likely to inspire positive action. And they shared that generic national advice on flooding is often met with “optimism bias”, where people assume the warning is for “the people who are at risk, it’s not me”. This highlights the need for messaging to more clearly articulate the risks to everyone.
Turner et al.’s (2024) analysis of two nationally representative surveys of older adults’ risk perceptions covering heat and cold provide a practical example of attending to message relevance in relation to labels. Findings suggest that older adults may respond better to guidance framed around peers (“people your age”) or situational markers (such as living alone) rather than age-related labels such as “65+”.
In relation to message content, several studies (Olson et al., 2023, Li et al., 2018; VanderMolen et al., 2022) suggest that segmented communications aimed at groups at heightened risk may be more effective when they make explicit the connection between the hazard and the factors that put someone at risk, supporting people to identify with and personalise the risk. However, content analyses of National Weather Service Twitter messages by both Olson et al. (2023) and Li et al. (2018) for example show that this kind of explanation, illustrated in Figure 3, is rarely included.
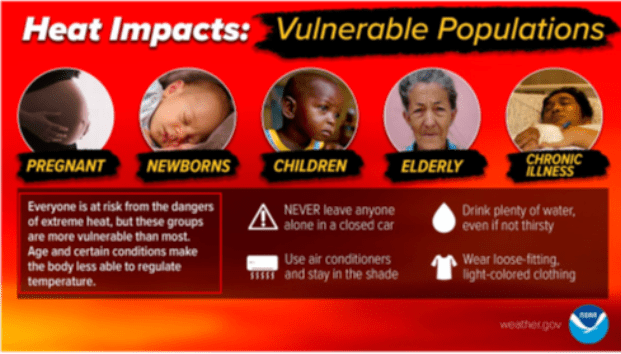
Figure 3: Heat warning image focusing on vulnerable populations (Source: Olson et al. 2023)
A qualitative study exploring barriers to heat communication (VanderMolen et al, 2022) aligns with this, recommending that communication interventions should help individuals understand and evaluate their risks with more specificity, as this improves willingness to adopt protective behaviours, for example, when people with chronic illness learn how their conditions increase heat sensitivity.
Olson et al. (2023) provide a further example of wording to illustrate this logic, linking individual or situational characteristics to a concrete mechanism of risk that people can recognise can make it more relevant and meaningful.
“Children cannot cool their bodies easily because they sweat less than adults. This puts them at higher risk for heat stroke, which includes nausea or vomiting, rapid heart rate, or death”. (Source: Olson et al., (2023)
Taken together, this evidence points to a consistent set of principles: avoid vulnerability labels that invite disengagement; use framing that considers how people self-identify/see themselves; recognise that different population segments may respond differently to the same message; and where targeting specific groups, support people to personalise the risk by explaining why they are vulnerable.
Relevance also relates to temporality. Because memories of heat discomfort weaken over time, timely, repeated reminders that link heat to discomfort or health impacts are recommended during the summer (Coombs et al, 2024;Health Canada, 2020). This aligns with research emphasising tailored messages to the phases of the emergency cycle (Tetzlaff et al., 2025b) and seasons (VanderMolen et al., 2022; Health Canada, 2020). This involves early-season communication, intensifying during events, and using the post-event period to reinforce messages, especially after heatwaves (Health Canada, 2020). For example, “we are still recovering from an extreme heat event, continue to drink cool water before you feel thirsty” (Health Canada, 2020). Repeating messages can boost protective intentions (Bruine de Bruin et al., 2016), and VanderMolen et al. (2022) recommend ongoing campaigns on adverse weather (heat).
Consider implications of socio-demographic differences
While socio-economic and socio-demographic factors do not predict risk behaviour, they are relevant for communicators because they shape people’s opportunity, means and motivation to act. This is why consistent implications for messaging, related to content (language, targeting and accessibility), channels and sources, emerge across the literature. This includes the importance of:
- Empowering people to act within their capabilities through clear, achievable actions.
- Acknowledging structural and systemic barriers, as advice that overlooks financial, housing or logistical realities risks sounding hollow, being perceived as irrelevant, and undermining trust. For example, telling low-income households to “seek cool spaces” (British Red Cross, 2023; Tetzlaff et al., 2025a) can feel unrealistic unless accompanied by information about available support and language that does not assume standard housing or resources.
- Ensuring equitable access to messages, especially for under-reached groups such as those with lower literacy or limited digital access.
- Noting that although gender does not predict behaviour on its own, consistently lower risk perception among men indicates a potential engagement gap.
Prosocial norms
Esplin et al. (2019) concluded that tailoring communication to the prosocial orientations of different population groups could strengthen engagement. For example, interactions with older adults can emphasise the need to take care of one’s health so they are able to help others effectively, and outreach with younger adults can encourage them to be more aware of vulnerable people around them and what they can do to help. However, because not everyone is embedded in strong social networks, messaging must avoid assuming access to family or community ties (Tetzlaff et al., 2025a).
Heat messaging example appealing to social norms (McLoughlin et al., 2023):
“Growing numbers of people are concerned about heat risks. At the same time, more and more people are taking actions to prepare themselves for heat risks, such as summer heatwaves.”
Summary: features of effective communication
The design of public health messages can support the acquisition of knowledge and awareness and (intended) protective behaviour if it acknowledges intervening factors and applies the following principles:
- Public health communication needs to include actionable guidance (e.g. drink 1.5–2l of water daily) which explains the rationale behind behaviours.
- Messages should start with verbs and specify concrete steps. Starting with verbs makes messages directive and concrete and increases their potential to affect behaviour change.
- Communicators need to pay attention to “message relevance”: people need to see themselves in the message and believe the message is for them. Broad public-facing communication may be more effective when risk is framed as relevant to “everyone”, rather than only to particular “vulnerable” groups. However, communication for groups at heightened risk still require more tailored approaches. This means considering how people self-identify, and explain why risk applies to particular people to support them to personalise the risk.
- Messages need to work with people’s emotional responses to adverse weather events and create messages that evoke emotions in line with the risk. Combining emotional appeals with efficacy information is more effective than appealing to emotions only.
- Content needs to be tailored to specific audiences, recognising diversity of communication needs, such as language and literacy needs, housing context, income, and geography. Messages should be kept simple and jargon free, using plain language and personal pronouns (“you”). Carry out readability testing, user testing with diverse groups. This is supported by reviews and good practice guidance.
- Language needs to be inclusive, simple, jargon free, and using personal pronouns. Storytelling can be used to deliver the message more effectively, for example through faith-based teachings or community gatherings. Images and infographics can further help people understand what to do and when.
- Timing of messages matters. Messages are more effective when sent close to an event and worded in phase with the emergency cycle.
Effectiveness of communication channels
Effectiveness of communications depends not only on what is communicated but also on how and through whom messages are transmitted. This dual aspect reflects the broader principle that effective communication must reach and resonate with diverse audiences. Communication channels influence reach and access, while the source shapes credibility, trust, and relatability (Coombs et al., 2024). These dimensions jointly affect whether individuals absorb information, perceive it as personally relevant, and translate it into protective behaviour.
The effectiveness of a communication channel can therefore be understood across two dimensions: reach, the extent to which people receive information; and whether exposure to a given channel is associated with changes in awareness, attitudes, or protective behaviours.
We did not identify studies that have directly tested the causal impact of different communication channels on attitudinal or behavioural outcomes. This limitation is confirmed across several evidence syntheses (Forsyth et al., 2023; Henderson et al., 2022; McIntyre et al., 2019; McLoughlin et al., 2023), which note a general paucity of comparative studies or evaluations that assess which types of channels or ‘messengers’ are most effective in changing behaviour. The result is a notable evidence gap.
This chapter synthesises findings from a subset of 21 of the 32 included items that discuss communication channels across heat (12), drought (3), mixed hazards (4) and floods (2). The dimensions covered include: channels typically used to disseminate adverse-weather information and patterns of access and preferences; how information is accessed or conveyed within a particular medium, with considerations on strengths and limitations in terms of reach and accessibility, with a smaller number of studies providing insights also into the type of information a particular channel can convey; and components of effective communication or factors affecting behaviour with related channel considerations.
Structured around the three main types of channels identified in the literature (traditional channels, digital channels, and social and community networks), this chapter synthesises findings across these three categories, supplemented by our stakeholder engagement discussions.
‘Traditional’ channels
Across all weather events, the evidence suggests that people still value communication via traditional, formal, or one-way channels. These include broadcast media such as TV and radio, and print media such as newspapers, brochures, and leaflets. Such channels have consistently been the most widely used and accessed sources of information on the risks of adverse weather events. This is true both in the UK (British Red Cross, 2023; Henderson et al., 2022; Lefevre et al., 2015) and internationally (Coombs et al., 2024; Health Canada, 2020; McIntyre et al., 2019; McLoughlin et al., 2023; Vu et al., 2019).
Recent UK data confirm this pattern. The 2023 British Red Cross survey on public perceptions of heatwaves found that 74% of respondents had heard about heatwaves from news or weather reports, 39% from the Met Office website, and 22% from local radio stations. Similarly, Henderson et al.’s review on flooding communication in Scotland (2022) highlights the important and well-evidenced role of broadcast outlets in reporting on extreme weather events and sharing practical advice before, during, and after flooding incidents.
These studies underline that traditional broadcast channels remain central to the dissemination of timely and wide-reaching public information, even if levels of trust in these outlets may be mixed (Coombs et al., 2024; McLoughlin et al., 2023).
Print materials, such as leaflets, brochures, and posters, already used in risk communication generally, also retain enduring relevance, particularly for older adults (Health Canada, 2020; Henderson et al., 2022; McIntyre et al., 2019; McLoughlin et al., 2023; Nitschke et. al., 2017; Williams et. al., 2019).
Our discussions with organisations supporting older adults similarly noted that concerns about online scams can make some reluctant to use digital platforms. Instead, older adults highly value physical communication methods such as posters and leaflets.
The advantages of print media lie in their accessibility, familiarity, and physical visibility. They can be distributed through mailings, local services, or community venues, allowing messages to reach people who may not actively seek information online. They can support increase in knowledge (Health Canada, 2020; Nitschke et. al., 2017) or act as prompts to remind people (particularly if they live alone) to adopt particular behaviours, such as drinking water during periods of extreme heat (Williams et. al., 2019).
Broadcast and print formats, therefore, remain effective channels for conveying public information during extreme weather events, including in Scotland (Henderson et al., 2022).
This has led some to recommend that organisations responsible for extreme-weather communication work more closely with the media and deliberately use multiple broadcast and print formats to maximise the reach of their messages (Henderson et al., 2022; McLoughlin et al., 2023; Oakman et al., 2010).
Digital channels: websites and social media
The rise of digital platforms has diversified communication pathways and enabled and empowered individuals to seek health and risk information independently (Coombs et al., 2024). The evidence on their impact on increasing awareness, knowledge, or protective behaviour is limited (Henderson et al., 2020; McLoughlin et al., 2023; McIntyre et al., 2019). However, there is some evidence on their respective strengths and limitations in terms of reach, accessibility, and the type of information they can convey.
Websites
Websites are among the channels most frequently used by public authorities to disseminate extreme weather information (McIntyre et al., 2019) and also rank among those most commonly accessed by the public, in the UK (British Red Cross, 2023; Henderson et al., 2022) and internationally (Tetzlaff et al., 2025a). As such, they represent an important component of communication strategies.
However, access is uneven. Henderson et al. (2022), for instance, point to low engagement with official (flood) websites, attributing this to preferences for face-to-face interaction, overconfidence in existing knowledge which discourages people from proactively accessing information, or limited information-seeking habits. Access also varies across social and demographic groups. Similarly, Coombs et al. (2024) observe that online use tends to differ by language, culture, and socioeconomic status, and a review of drought-related vulnerability in Scotland illustrates this digital divide: while 93% of households report internet access, this falls to 87% in the most deprived areas, compared with 99 % in the least deprived (McClymont et al., 2020). Although online platforms extend the reach of public information, they cannot ensure equitable exposure or engagement across all population groups.
Four studies provide information related to the content that websites can provide. In their reviews of communication practices in hazard and emergency contexts, Henderson et al. (2022) and Coombs et al. (2024) identify websites as particularly valuable for delivering clear, practical, and comparatively detailed information. In contrast to social media, which have character and format limitations, websites can accommodate comprehensive guidance, explanatory content, and links to additional support resources (Coombs et al., 2024). This finding is supported by two heat-related channel-specific studies (social media and websites), both of which highlight the limitations that platform design creates on message depth (Olson et al., 2023; Tetzlaff et al., 2025a).
Tetzlaff et al. (2025a) offer a useful illustration of how channels with differing capacities can be combined. Although the study focused on Environment and Climate Change Canada’s national heat-health alert system, outside the scope of this review, and did not include behavioural outcome data, it provides a useful and transferable example of cross-channel design. It shows how concise messaging can be paired with web-based resources to extend depth.
Layered communication in Canada’s heat-health messaging system
To help educate the public during heat events, Health Canada and Environment and Climate Change Canada (ECCC) distribute heat-health messaging through national weather warning messages. Because these messages must be concise and suitable for a national audience, they face inherent challenges in providing sufficient detail or tailoring for specific risk groups.
To address this, Health Canada and the ECCC implemented a layered communication design in which the brevity required by the alert format was mitigated by hyperlinks directing readers to Health Canada’s website for more detailed, context-specific advice. The alerts provided short, actionable statements (e.g., reminders to “stay hydrated”), while the linked webpages elaborated on these actions, offered more detailed practical guidance, and included additional materials tailored for specific populations, illustrating the broader principle that websites can act as ‘anchors’ for more detailed content within a layered communication system.
Some specifically caution that the advantages of websites can be offset by weaknesses in design, readability, and accessibility. For instance, websites can be text-heavy, outdated, or poorly structured, making it difficult for users to navigate and absorb key messages (Henderson et al., 2022; Tetzlaff et al., 2025b). Tetzlaff et al.’s (2025b) readability assessment of local authority heat-related web pages in Canada found that much of the online material was pitched at a level too complex for the general public to understand. These barriers can also discourage repeat visits and reduce the visibility and usability of essential health advice.
These findings emphasise that ongoing investment in digital infrastructure and a sustained focus on accessibility are essential to maximise their benefits. At the same time, while websites remain valuable for providing detailed reference material, they should not be relied upon as the sole vehicle for inclusive health messaging. Public bodies must also recognise uneven digital access when designing communication strategies, ensuring that information reaches those who need it most and reflects communities’ preferred sources of information.
Social media platforms
Social media platforms (e.g., X, Instagram) are increasingly used to disseminate information about adverse weather and health risks and are now an established yet still-evolving component of this communication landscape (Henderson et al., 2022; McIntyre et al., 2019; Vu et al., 2019). Some organisations, for example the Red Cross and YMCA, are taking the lead in social media, disaster preparedness and health adaptation. They offer speed, immediacy, and potential for interactive engagement (McIntyre et al., 2019).
Social media use is highest among younger demographics (British Red Cross, 2023; Olson et al., 2023), creating opportunities to reach audiences that may not typically engage with more traditional channels such as broadcast or print media. However, as with websites, access and audience reach are uneven. Olson et al.’s (2023) study of heat-risk communication on Twitter in the United States for example specifies that only around 7% of Twitter users were aged 65 or older, limiting the platform’s direct reach to those most vulnerable to extreme heat. Nonetheless, the authors note that such channels could still play an indirect role by reaching younger caregivers and family members who may act as intermediaries for at-risk older adults.
Social media platforms have structural constraints, such as character limits, that can make it difficult to convey detailed information (Coombs et al., 2024; Olson et al., 2023; Tetzlaff et al. 2025a). Indeed, Olson et al. (2023) acknowledge this limitation within their broader argument that to persuade people to act, messaging needs to convey additional kinds of information (for example, justifying why a behaviour is recommended), as highlighted in the previous chapter. They therefore suggest using images, infographics, and ‘threaded’ messages to expand content. This design logic mirrors the layered communication approach illustrated by Tetzlaff et al. (2025a), where prioritisation i.e. focusing on essential, actionable advice, and cross-linking to web-based material was used to offset these limitations. This principle is directly applicable to social media practice, where posts can link to more detailed resources, use visual elements to enhance comprehension, and tailor messaging for different audiences.
Our stakeholder engagement provides examples of how these channels operate in practice across national, regional, and local contexts in Scotland.
Discussions we had with organisations in Dumfries and Galloway highlighted how different parts of Scotland’s communication infrastructure function together across scales. Locally, the Grow Well app delivered through Healthzone is widely used and trusted by parents, has been used for messaging around storms, with potential to extend information to other weather events.
Early years organisations we spoke to also make use of national resources such as Parent Club, viewed as a reliable source of advice to share with families, and of social media platforms like Facebook to communicate with parents, though there is uncertainty about how effective these are. Participants in our stakeholder engagement activities also pointed to hyperlocal channels, such as the “Edinburgh Minute” community news board, which frequently shares weather warnings within neighbourhood networks.
These discussions also highlighted the practical constraints that shape channel use. Digital-only dissemination is often unavoidable due to considerations around costs of producing printed leaflets or posters.
Digital resources like the NHS Inform webpages on summer health and heat safety were valued for being concise, accessible, and easy to navigate, offering short prompts, bullet-pointed guidance, and links to further information.
Social and community networks
A parallel layer of communication operates through community-embedded routes. These include both formal intermediaries, such as carers, doctors, and other healthcare professionals, local civil society organisations, community or faith leaders, schools, and social landlords, and informal networks of friends, neighbours, peers, and family members who exchange information through everyday interactions and ‘word of mouth’ (British Red Cross, 2023; Coombs et al., 2024; Forsyth et al., 2023; Health Canada, 2020; McIntyre et al., 2019; McLoughlin et al., 2023; VanderMolen et al., 2022; Williams et al., 2019).
The contribution of community-embedded routes lies in how they activate mechanisms that can influence behaviour: credibility and trust; amplification and reach; and relevance.
First, as discussed in Chapter 5, trust shapes whether advice is perceived as credible. Trusted figures include official or expert institutions, such as meteorological agencies (e.g. the Met Office), climate scientists, public health bodies, and weather forecasters (McLoughlin et al., 2023). However, local or community-based organisations and intermediaries, such as healthcare staff, community leaders, and faith organisations, are often trusted because of familiarity, accessibility, and ongoing relationships (Health Canada, 2020; McIntyre et al., 2019; McLoughlin et al., 2023; VanderMolen et al., 2022). Fathollahzadeh et al. (2023) describe this as the product of long-term credibility and perceived reliability. Williams et al. (2019), for example, found that carers and healthcare staff were often the primary conduits of heat-health information for older adults. These figures are perceived as credible and knowledgeable, which increases the likelihood that messages and recommended actions will be believed and acted upon (Coombs et al., 2024; Health Canada, 2020; McIntyre et al., 2019; Tan et al., 2024; VanderMolen et al., 2022).
Organisations representing older adults and those with long-term health conditions we spoke to as part of our engagement activities highlighted that the person who disseminates the public health messaging is also important, not just the message being given. They described that the person giving advice needs to be trusted, and co-produce messages with the communities they’re trying to reach.
Chapter 5 also highlighted the role of social norms in shaping protective behaviour. Community networks, which also include peers, friends, family, and neighbours, provide one of the main mechanisms through which these influences operate in practice. Forsyth et al.’s review of barriers to flood communication (2023), for example, notes that “the most powerful preparedness spokespersons are not government agencies or nongovernment organisations but simply other community members who have prepared” (p. 122). McLoughlin et al.’s review of determinants of heat-health behaviours (2023) and Tan et al.’s review of motivational factors influencing responses to mixed hazards (2024), including floods, further observe that trusted organisations can reinforce these social influences by modelling and endorsing protective behaviours within the community.
These findings resonate with insights from our stakeholder engagement discussions and build directly on the patterns highlighted in Chapter 5 regarding boys’ and young men’s low risk perception during hot weather. While these young men often dismiss formal messaging about sun exposure or dehydration, staff from a youth organisation noted that they were more receptive when safety guidance was shared informally by adults they knew and trusted, especially when those adults modelled the behaviours themselves, such as applying sunscreen.
Second, and relatedly, intermediaries enhance effectiveness by extending reach and raising awareness while reinforcing and validating ‘official’ information (McLoughlin et al., 2023). This amplification capacity can ensure that information reaches people who might otherwise be missed, either because they are less engaged with formal or digital media, or because some may distrust ‘official’ sources (British Red Cross, 2023; Coombs et al., 2024; McIntyre et al., 2019; VanderMolen et al., 2022).
Some international evidence shows intermediary networks can bridge gaps in reach and awareness. McLoughlin et al. (2023) found that mobile nurse outreach effectively delivered heat-health advice to older adults in Austria, helping close awareness gaps among vulnerable groups. VanderMolen et al. (2022) reported that low heat risk awareness was common among those with multiple vulnerabilities, such as age, limited education, or social isolation, and noted that community organisations are well placed to address these gaps. Both studies conclude that communication can be more effective through intermediaries with established contacts than direct outreach. Weitkamp et al.’s UK-based participatory research on challenges of communicating drought risk to the public (2020) reaches a similar conclusion (with a focus on water use). In the UK, because drought is seen as remote (‘drought happens elsewhere’) and inconsistent with lived experience, it creates ‘psychological distancing’ that reduces its perceived relevance. The study suggests that intermediary groups with emotional or experiential ties to water and the environment can help bridge this gap by acting as spokespeople or ‘multipliers’, extending message reach and resonance.
Insights from our stakeholder engagement activities reflect these patterns, highlighting how intermediaries can also convey information in culturally relevant ways, for example, using faith as an ‘entry point’.
Organisations working with diverse communities emphasised the central role of religious institutions (mosques and gurdwaras) can act as information hubs, reaching people across generations, including older adults who may have limited English proficiency or digital access. Trusted faith and community leaders can communicate public health information in culturally relevant and meaningful ways, for example by embedding it in religious teachings.
Third, community networks, who bring knowledge of needs and target audiences and local areas, can enhance personal relevance (Coombs et al., 2024; Health Canada, 2020; McLoughlin et al., 2023; VanderMolen et al., 2022; Weitkamp et al., 2020) through their ability to adapt public health guidance to lived realities, making it accessible and actionable by tailoring advice to people’s specific needs and circumstances, factors repeatedly identified as prerequisites for behavioural change.
This is because community networks can also provide unique opportunities for face-to-face or two-way exchanges, which allow individuals to ask questions, clarify advice, and relate general guidance to their lived experience. VanderMolen et al. (2022) illustrate how such dialogic exchanges increase comprehension and awareness of risk and heat-protective behaviours, their perceived relevance and confidence to act. These findings are consistent with several evidence reviews exploring the effectiveness of public- health disaster and extreme weather communication beyond heat (e.g. floods), which highlight that interactive, relational communication outperforms one-way information transfer for these reasons (Coombs et al., 2024; Henderson et al., 2022; McIntyre et al., 2019).
An example from our stakeholder engagement discussions illustrates this mechanism.
An organisation working with diverse communities runs interactive sessions that use discussion and guided questions to raise awareness of climate and adverse-weather risks in the Scottish context. This is because while many recognise the impacts of adverse weather (for example, flooding or drought) in their home countries, they may not realise that these events can and do occur in Scotland. By using real incidents as discussion prompts and encouraging people to talk through how they might respond, these sessions deepen understanding of adverse weather risks and make protective actions feel more concrete.
Two heat-focused studies emphasise that these actors can benefit from guidance and support to perform their roles effectively. Based on qualitative research involving community leaders, health workers, and representatives from public and third-sector organisations, VanderMolen et al. (2022) highlight that these intermediaries are part of established communication networks and outreach efforts. While well-positioned to convey public health messages, participants pointed out the need for training and expert input to equip them with the knowledge and confidence to educate their communities and train others. Similarly, McLoughlin et al. (2023) mention the potential of building capacity among diverse communicators, such as weather presenters, journalists, and community educators. They cite existing initiatives such as the Climate Matters programme in the U.S., which offers targeted training and resources, and UK initiatives such as the Women’s Institute, which has trained its members in heat risk communication.
Community networks are therefore conceptualised not as substitutes for formal channels, but as complementary components of a diversified communication strategy, where multi-channel delivery emerges as an important feature of communication effectiveness (British Red Cross, 2023; Coombs et al., 2024; Fathollahzadeh et al., 2023; Forsyth et al., 2023; Health Canada, 2020; Henderson et al., 2022; McIntyre et al., 2019; VanderMolen et al., 2022; Vu et al., 2019; Weitkamp et al., 2020).
This also points to the importance of consistency across message senders. Weitkamp et al., (2020) provide a practical illustration of contradictory guidance in relation to drought, where water companies may advise the public to conserve water while public health bodies simultaneously urge people to drink plenty of fluids (as drought is likely associated with a heatwave), highlighting a need for “careful management of the message” (p.842). Other studies also point out that contradictory information may undermine credibility and trust, create confusion, and weaken engagement with protective advice (Coombs et al., 2024; Fathollahzadeh et al., 2023; Forsyth et al; Health Canada, 2020).
Features of effective communication channels
The evidence presented in this chapter highlights that different types of communication channels (traditional, digital, and community-based) have different strengths and characteristics. These underpin the following overarching features of effective communication that emerge consistently across the literature:
No single channel is sufficient on its own. Maximising reach and accessibility requires diversifying channels, blending ‘traditional’ and digital media, and including community networks to maximise exposure to information.
Consistency across channels and senders is important. Conflicting messages can erode public trust, create confusion, and reduce compliance.
Communication strategies must be tailored with attention to equity of access, accounting for variations in digital connectivity, literacy, language, and cultural context.
Trust in the source increases message effectiveness. Messages are more likely to be acted upon when they come from credible, relatable, and trusted communicators.
Beyond broad cross-cutting features, below are channel-specific considerations presented in this section:
Traditional channels such as broadcast media and print materials remain valuable for disseminating information. Given their wide reach and continued use, some studies recommend that public health agencies strengthen collaboration with media outlets and intentionally use a mix of broadcast and print formats to maximise coverage.
Websites are widely used sources of information, while social media platforms are increasingly used to disseminate adverse-weather and health information. However, access, engagement, and audience reach remain uneven across population groups. They bring distinct strengths and design requirements. Websites can act as reference points, and their strength lies in their ability to provide clear and relatively detailed information. To make the most of them, attention should be given to content clarity, accessibility and usability. Poor design, inaccessible formats, or out of date content can reduce engagement. Social media can provide speed and visibility, reaching younger demographics particularly. Although it has structural limitations (e.g. limited characters), these can also be offset by layered communication, where brief posts link to more comprehensive resources. Infographics, videos, and visual aids can improve clarity and appeal.
Social and community networks can extend reach, improve comprehension, increase perceived relevance, and build confidence in recommended actions, particularly among groups considered to be at greater risk and/or less likely to engage with ‘official’ sources.
Links to wider evidence
We find that effective public health communication on adverse weather is well aligned with disaster risk communication and the risk perception literature generally (Fathollahzadeh et al, 2023; Speilhofer et al., 2020).
Stead et al. (2019) explored the use of media to communicate public health messages in six health topic areas (alcohol, diet, illicit drugs, physical activity, sexual and reproductive health and tobacco). The authors found that, depending on the topic area, mass media campaigns can influence knowledge, attitudes and beliefs, lead people to seek help and change behaviour (physical activity topic only). In line with our findings, this systematic review also found that targeting messages can be effective.
They also found some evidence that negative or ‘hard-hitting’ messages, as well as those aiming to shift social norms, may lead to behaviour change. There was also some evidence that both positive and negative messages can be effective, depending on the topic. Our rapid review suggests that the effectiveness of such messages related to adverse weather is more nuanced. For example, evoking emotions needs to be accompanied by actionable guidance; in relation to social norms, some studies suggest that messages which emphasise what others do or approve of can help normalise protective behaviours.
Reflecting the different characteristics of weather and the six health topics Stead et al. investigated, they found that “campaigns that run for longer and are more intensive (with people exposed to them more often, for example) are likely to be more effective, based on evidence from tobacco and sexual health campaigns in particular”. For communicating health risks of extreme weather events, and heat in particular, our findings also stress temporal proximity to an adverse weather event, the need to adjust messaging accordingly and repetition.
Conclusions
The evidence base on the effectiveness of public health communication for adverse weather events is limited. Only three studies identified in this review were designed to measure behavioural and health outcomes in ways that allow causal inference. All three were related to heat and specifically designed to target vulnerable groups (older adults and those with chronic conditions). The evidence suggests that public health communication can contribute to behaviour change.
The larger body of evidence we reviewed looks at how people respond to public health messages in real-world settings; for example whether they notice messages, remember advice, report changing (or intending to change) their behaviour. They also explore the factors that influence whether they act or intend to act. Across these studies, findings suggest that changes tend to be modest and not consistently observed among those considered most vulnerable, who may not be reached by public health messages or do not act on them. The pathway towards behaviour change is therefore non-linear and shaped by a range of individual and contextual factors.
The two main explanations around which there is broad alignment in the literature are:
People (in particular older people) do not like to see themselves as vulnerable, hence do not accept that they need to change behaviour.
People need to believe that the recommended actions are effective (response efficacy) and achievable (self-efficacy) to adopt them. They also need to believe that their actions can make a difference.
Other reasons include: not remembering or understanding the message; positive emotional responses evoked by mentioning of weather events (in the UK especially heat); practical barriers to implementing recommended actions.
Evidence from the wider risk perception literature shows that direct experience of a weather event, especially if negative and recent, shapes people’s perceived risk/sense of vulnerability and action, often more powerfully than information alone. Social influences (norms and interpersonal interactions) shape an individual’s adaptive behaviour, especially when people feel they have control. However, socio-demographic and socio-economic factors do not reliably predict how people perceive weather related health risk and their behaviour responses as these factors interact with psychological and contextual mediators.
The literature points to the importance of designing communications with attention to the contextual and individual factors that shape behavioural responses.
Effective messages tend to share several common features:
Practicality supports uptake. Effective messages are often action-focused, specific and feasible, using language that feels relevant and understandable to intended audiences. Clear steps, explained in straightforward terms and supported where appropriate by visuals or simple formats, help people understand both what to do and why it helps.
People engage with advice when they can interpret it, recall it, see why it matters, and recognise that the recommended actions fit their circumstances: messages that explain why an action is recommended appear to support people in assessing its value, while recognition of financial, physical, or practical constraints is associated with higher perceived realism.
Relevance and clarity shape how messages land. Tailoring content to different audiences and using plain, inclusive language — while avoiding labels that many at-risk individuals do not identify with — is also associated with greater relevance and engagement as it increases understanding and resonance.
Effectiveness of adverse-weather communication depends as much on how messages travel as on what they say. We did not identify studies that have tested the causal impact of different communication channels on attitudinal or behavioural outcomes, which reflects a gap in the evidence base. There is more consistent evidence regarding the types of channels used to disseminate adverse-weather information, patterns of access and preference, and their strengths and limitations. This includes reflections drawn from behavioural studies around what may make channels effective.
Three overarching conclusions stand out:
Different channels play different roles, and no single route reaches everyone.
Traditional broadcast and print media still provide the widest reach; digital platforms offer speed and detail but do not engage all groups; and community and social networks can add trust, credibility, and opportunities for dialogue. Effective communication draws on these complementary strengths rather than relying on a single medium.
Trust and relevance shape how messages are received. People are more likely to pay attention and act when information comes from sources they recognise and rely on -whether national institutions, local organisations, or familiar community figures. Consistency across channels and senders helps maintain credibility and avoids confusion.
Equity of access affects exposure and response. Not everyone encounters information in the same way. Differences in digital access, literacy, language, and social support influence who hears a message and how they interpret it. Combining mass-reach channels with community-embedded routes can help ensure that those most at risk are not missed.
Future research
Research on public health communication is limited for weather events beyond heat and for vulnerable groups other than older adults e.g. young people, whose behaviour changes could yield long-term benefits. Few studies robustly evaluate messaging beyond self-reports or participatory planning, and author-devised messages are rarely user-tested. Comparative evidence on how people access information and the outcomes of different communication channels is also lacking. The role of misinformation or disinformation in shaping public responses to adverse weather is an important area of concern, particularly in the context of social media, and we note it as an area for further exploration.
References
Adaptation Scotland (2025): Climate projections for Scotland – summary (https://adaptation.scot/scotland-and-climate-change/climate-change-trends-and-projections/).
Antwi, S.H., Rolston, A., Linnane, S. and Getty, D., (2022). Communicating water availability to improve awareness and implementation of water conservation: A study of the 2018 and 2020 drought events in the Republic of Ireland. Science of the Total Environment, 807, p.150865.
British Red Cross (2023): Policy Brief: public perceptions of heatwaves in the UK
Bourret Soto, M. and Guillon, M., (2024). What drives adaptive behaviours during heatwaves? A systematic review with a meta-analysis. Climate Policy, 24(8), pp.989-1003.
Bruine de Bruin, W., Lefevre et al., 2015, C.E., Taylor, A.L., Dessai, S., Fischhoff, B. and Kovats, S., (2016). Promoting protection against a threat that evokes positive affect: The case of heat waves in the United Kingdom. Journal of experimental psychology: applied, 22(3), p.261.
Climate Change Committee (2021): Evidence for the third UK Climate Change Risk Assessment – Summary for Scotland
Coombs, N.M., Porter, J.E. and Barbagallo, M., (2024). An exploration of the influencing factors for effective public health messaging during disasters: a scoping review. Public health, 228, pp.73-81.
Cullen, J., Drabble, D., Parry-Crooke, G., Junge, K.; Hastings-Caplan, R., Corran, Ph. (2019). Mapping the Evolving Digital Inclusion landscape to support Cohesion and Integration – Deliverable D2.2. Evidence Effectiveness and Replication Potential Tool.
Devane, D., Hamel, C., Gartlehner, G., Nussbaumer-Streit, B., Griebler, U., Affengruber, L., Saif-Ur-Rahman, K.M. and Garritty, C., (2024). Key concepts in rapid reviews: an overview. Journal of Clinical Epidemiology, 175, p.111518.
Erens, B., Williams, L., Exley, J. et al. (2021): ‘Public attitudes to, and behaviours taken during, hot weather by vulnerable groups: results from a national survey in England’. BMC Public Health 21, 1631
Esplin, E.D., Marlon, J.R., Leiserowitz, A. and Howe, P.D. (2019). “Can you take the heat?” Heat-induced health symptoms are associated with protective behaviours. Weather, climate, and society 11(2), pp.401-417
Fathollahzadeh A, Salmani I, Morowatisharifabad MA, Khajehaminian MR, Babaie J, Fallahzadeh H. (2023). Models and components in disaster risk communication: A systematic literature review. Journal of education and health promotion. Mar 1;12(1):87
Forsyth, W., Roberts, T., & Brewer, G. (2023). Conceptualising risk communication barriers to household flood preparedness. Urban Governance, 3(2), 116-129.
Global Water Partnership (2019). How to communicate Drought A guide by the Integrated Drought Management Programme in Central and Eastern Europe.
Health Canada: Water, Air and Climate Change Bureau Healthy Environments and Consumer Safety Branch (2011; updated in 2020). Communicating the Health Risks of Extreme Heat Events: Toolkit for Public Health and Emergency Management Officials
Henderson, F., Helwig, K. and Teedon, P., (2022). Effective future communication of flood risk in Scotland.
James Hutton Institute (2023): Summary for Policy Makers: Climate trends, future projections and extremes and their implications for Natural Capital and policy
Lefevre, C.E., Bruine de Bruin, W.B., Taylor, A.L., Dessai, S., Kovats, S. and Fischhoff, B., (2015). Heat protection behaviours and positive affect about heat during the 2013 heat wave in the United Kingdom. Social Science & Medicine, 128, pp.282-289.
Li, Y., & Howe, P. D. (2023). Universal or targeted approaches? An experiment about heat risk messaging. Natural Hazards, 117, 381–398.
Li, Y., Hughes, A.L. and Howe, P.D., (2018). Communicating Crisis with Persuasion: Examining Official Twitter Messages on Heat Hazards. In ISCRAM.
McClymont, K. and Beevers, L. (2022). Understanding the social factors influencing resilience to drought exposure in Scotland: CREW Policy systematic review. CRW2020_19 CREW Policy Fellowships Programme: Scotland’s Centre of Expertise for Waters (CREW).
MacIntyre E, Khanna S, Darychuk A, Copes R, Schwartz B (2019): Evaluating risk communication during extreme weather and climate change: a scoping review. Health Promot Chronic Dis Prev Can. 39(4):142-156.
McLoughlin, N., Howarth, C. and Shreedhar, G., (2023). Changing behavioural responses to heat risk in a warming world: How can communication approaches be improved? Wiley Interdisciplinary Reviews: Climate Change, 14(2), p.819.
Mehiriz, K., Gosselin, P., Tardif, I., & Lemieux, M. A. (2018). The effect of an automated phone warning and health advisory system on adaptation to high heat episodes and health services use in vulnerable groups—evidence from a randomized controlled study. International journal of environmental research and public health, 15(8), 1581.
Nitschke M, Krackowizer A, Hansen AL., Bi P, Tucker GR (2017): Heat Health Messages: A Randomized Controlled Trial of a Preventative Messages Tool in the Older Population of South Australia. Int J Environ Res Public Health, Aug 31;14(9):992.
Oakman, T., Byles‐Drage, H., Pope, R., & Pritchard, J. (2010). Beat the Heat: don’t forget your drink–a brief public education program. Australian and New Zealand journal of public health, 34(4), 346-350.
Olson, M. K., Sutton, J., & Waugh, N. (2023). Tweeting the Heat: An Analysis of the National Weather Service’s Approach to Extreme Heat Communication on Twitter. Weather, Climate, and Society, 15(4), 963–976.
Public Health Scotland (2024): Protecting the population from the negative health and wellbeing impacts of adverse weather: Public Health Scotland plan 2024-2027
Ratwatte, P., Wehling, H., Kovats, S., Landeg, O., & Weston, D. (2022). Factors associated with older adults’ perception of health risks of hot and cold weather event exposure: a scoping review. Frontiers in public health, 10, 939859
Sayers, P., Lindley, S., Carr, S. and Figueroa-Alfaro, R., (2023). The impacts of climate change on population groups in Scotland.
Scottish Government (2025): The Scottish Health Information Integrity Strategy 2025-2030. Available at: https://www.gov.scot/publications/scottish-health-information-integrity-strategy/documents/
Spielhofer, Th., Junge, K., Cullen, J. Allen, R., Iacopini, G., Hahne, A., Laterza, R., Ferrari, O., Dimitrov, Y., Miteva, N., Veleva, V., Kostoulas, I., Didachos, M. (2020). Analysis on Risk Perception, Deliverable D2.1 of the RESILOC project (unpublished)
Stead M, Angus K, Langley T, Katikireddi SV, Hinds K, Hilton S, et al. (2019).Mass media to communicate public health messages in six health topic areas: a systematic review and other reviews of the evidence. Public Health Res 2019;7(8)
Takahashi, N., Nakao, R., Ueda, K., Ono, M., Kondo, M., Honda, Y., & Hashizume, M. (2015). Community trial on heat related-illness prevention behaviors and knowledge for the elderly. International journal of environmental research and public health, 12(3), 3188-3214.
Tan, H., Hao, Y., Yang, J. and Tang, C., (2024). Meta-analyses of motivational factors of response to natural disaster. Journal of environmental management, 351, p.119723.
Tetzlaff, E.J., MacDonald, M., Kenny, G.P., Murphy, B., Siblock, R.F., Al.-Hertani, A., Stranberg, R.C., Berry, P. and Gorman, M., (2025a). Updating Health Canada’s Heat-Health Messages for the Environment and Climate Change Canada Heat Warning System: A Collaboration with Canadian Experts. International journal of environmental research and public health, 22(8), p.1266.
Tetzlaff, E. J., Wagar, K. E., Johnson, S. J., Gorman, M., & Kenny, G. P. (2025b). Heat-health messaging in Canada: A review and content analysis of public health authority webpages and resources. Public Health in Practice, 9, 100576.
Turner, G.A., Moreira de Sousa, A., O’Connell, E., Kovats, S., Brooks, K., Landeg, O., Ismail, S., Rajamani, A. and Hajat, S., (2024). Health perceptions of adverse weather in older adults in England: analysis of 2019/20 survey data. European journal of public health, 34(6), pp.1192-1198.
UK Health and Security Agency (2024). Adverse Weather and Health Plan – supporting evidence
UK Health and Security Agency (2023). Health Effects of Climate Change (HECC) in the UK. State of the Evidence, 2023
VanderMolen, K., Kimutis, N. and Hatchett, B.J., (2022). Recommendations for increasing the reach and effectiveness of heat risk education and warning messaging. International Journal of Disaster Risk Reduction, 82, p.103288.
Vu, A., Rutherford, S. and Phung, D., (2019). Heat health prevention measures and adaptation in older populations—a systematic review. International journal of environmental research and public health, 16(22), p.4370.
Wachinger, G., Renn, O., Begg, C. and Kuhlicke, C. (2013). The risk perception paradox—implications for governance and communication of natural hazards. Risk analysis, 33(6), pp.1049-1065.
Weitkamp, E., McEwen, L. and Ramirez, P., (2020). Communicating the hidden: Toward a framework for drought risk communication in maritime climates. Climatic Change, 163(2), pp.831-850.
Williams, L., Erens, B., Ettelt, S., Hajat, S., Manacorda, T. and Mays, N., (2019). Evaluation of the heatwave plan for England.
Appendices
This study was delivered in two main phases. Phase 1 consisted of a Rapid Evidence Review (RER), which identified, assessed, and synthesised existing evidence on public-health communication and behavioural responses to adverse weather events (heat, cold, flooding, and drought). Building on Phase 1, Phase 2 consisted of an engagement phase involving interviews and workshops with key stakeholders.
This Appendix describes the detailed methodology for each phase.
Phase 1: Rapid Evidence Review: overview
The RER is a pragmatic and streamlined literature review method designed to collect and synthesise the best available evidence to support decision-making in a timely way (Devane et al. 2024). While RERs are not as comprehensive as systematic reviews, both approaches share robust, replicable and transparent methodologies. The key advantage of the RER approach lies in its pragmatism, making it particularly suitable for producing policy-relevant insights within short timeframes. We describe the stages of the review in the next sections.
Inception and scoping
The inception and scoping phase began with three scoping interviews with people with expert insight on our research questions. These interviews deepened our understanding of the policy context within which this research is situated.
Next, we developed search terms and a set of primary inclusion and exclusion criteria to guide the evidence search process. We included studies relating to the four weather events in scope (heat, cold, flooding, and drought) and prioritised those that focused on Scotland and the wider UK, along with comparable countries, defined here as high-income nations with institutional capacity for public health communication, broadly similar exposure to climate-related weather risks, or comparable temperate climates. These included North America, Western and Northern Europe, Australia, and New Zealand. We included only publications in English from between 2015 and 2025. We selected the starting point of 2015 to balance breadth and relevance within the constraints of a rapid review methodology. The date range reflects the growing research focus on climate resilience over the past decade, while ensuring the volume of literature remained manageable and timely for synthesis.
We then agreed secondary criteria and piloted the search to guide the literature screening process. The criteria were designed to assess both relevance and quality, capturing geographic fit, attention to health outcomes, inclusion of messaging examples, alignment with phases of the disaster-management cycle (preparedness, response, recovery) and study quality.
Formal search, longlisting and screening
The formal search proceeded in two waves. The first covered three bibliographic databases—Web of Science, ProQuest, and PubMed—using the refined search strings developed during inception. We applied the primary criteria to screen titles and remove clearly non-relevant items. We applied the secondary criteria at abstract and full-text stages. The second wave consisted of targeted searches for grey literature using Google and Google Scholar to address evidence gaps.
The final sample comprised 32 studies: 26 peer-reviewed articles and six grey literature reports. Most items focused on heat (n = 20), with a comparatively smaller number addressing both heat and cold (n = 2), drought (n = 4), floods (n = 2), multiple hazards (n = 4), which included heat and / or floods alongside other extreme weather events that were out of scope. In terms of geographic coverage, studies covered the UK (9) followed by the USA (5), Canada (4) and Australia (2). Evidence syntheses generally drew on broader international evidence.
We retained two literature items that fell outside the predefined geographic range. One study, from Japan, was included because it provided robust outcome data on a communications intervention. The second, focused on Central and Eastern Europe, was included due to its relevance to drought-related communication – a drought communication guide developed by a network of organisations from multiple countries, and based on available literature and relevant evidence.
Appendix C contains the full list of documents included in the review.
Data extraction and synthesis
We extracted information from each literature item using a structured template developed in Microsoft Word (Appendix B). The template drew on established frameworks for effective disaster risk communication and risk perception (Fathollahzadeh et al., 2023; Spielhofer et al., 2020) and was adapted to reflect the specific research questions for this study. Each member of the research team piloted the template to ensure consistency and fitness for purpose.
We organised the extracted data in MAXQDA, a qualitative analysis software package, and undertook thematic coding and synthesis, which we supplemented with data from the engagement phase (section 10.3 below).
Rapid Evidence Review: detailed approach
Following established principles, we conducted the RER in four main stages: (1) search strategy and piloting (conducted as part of the project’s scoping and inception); (2) longlisting; (3) screening and shortlisting; (4) extraction and synthesis.
Stage 1: Search strategy and piloting
This stage took place during the project’s inception. It involved developing search strings, inclusion and exclusion criteria, and piloting of search terms across selected databases. Initially, the plan was to search two databases (PubMed and ProQuest) alongside Google/Google Scholar. However, piloting showed that open-web searches generated an unmanageable volume of ‘hits’. Consequently, we slightly re-oriented our approach to include a third database (Web of Science) and to separate the process into two waves: peer-reviewed literature searches; and targeted grey-literature searches conducted at a later stage to fill evidence gaps. This refinement enabled a more efficient approach without compromising the feasibility of screening within a rapid review timeframe.
For research questions 1 and 2, we developed search terms using combinations of keywords across four core conceptual domains: weather events, communication, health outcomes, and effectiveness. To enhance the search design, we used SciSpace GPT, an AI-based research tool, to identify additional synonyms and related terms, which were incorporated into the final search strings. Although emergency alerts / warning systems were not within the formal scope of the review, we retained these terms in the search strategy to avoid restricting the evidence base and to capture studies that might offer transferable insights for public health communication more broadly. We then used the second-stage screening process to identify and retain studies that contained findings relevant to wider communication practice. Table 1 illustrates the resulting set of search terms.
Weather event | Communication | Health outcome | Effectiveness |
|---|---|---|---|
Heatwave*, “extreme heat”, “high temperature*”, “hot weather”, “extreme heat events” | “risk communication*”, “communicat*”, “persuasive communication*”, “public health communication*”, “risk messag*””public health warning*”, “emergency alert*” | Awareness, “behavioural response”, “health behaviour*”, “behaviour change”, compliance, adaptation, “health outcome*”, “public health outcome*”, “population health outcome*”, impact, “public health impact”, “population health impact”, “heat related illness”, “health risk”; mortality; morbidity | Evaluation; effectiveness |
“extreme cold”, “cold spells”, “cold weather”, “severe cold temperature*” | As above | As above, cold related illness | As above |
Flood*, “flood event*”, “river flood”, “flash flood”, “coastal flood”, “surface-water flood”, “fluvial flood”, “pluvial flood” | As above | As above | As above |
Drought*, “water shortage”, “water scarcity” | As above | As above | As above |
Table 1: Questions 1 and 2 search terms
The terms were combined using Boolean operators (AND/OR) and adapted for each database. An example ProQuest search string for heat-related studies was structured as follows: (“heatwave” OR “heat wave” OR “extreme heat” OR “extreme heat events” OR “high temperatures”) AND (“risk communication” OR “public health communication” OR “public health warning*” OR “emergency alert *” OR “risk messag*”) AND (“health risks” OR “heat-related illness” OR “public health impact” OR “public health outcome*”).
Searches targeted terms in titles and abstracts, ensuring that generic terms such as “extreme weather” or “adverse weather” were also captured. Additional variants were therefore unnecessary.
For research question 3, we applied a more streamlined search. Given the size and maturity of the literature on factors influencing risk perception and behaviour in disasters, the search was designed to capture the strongest available evidence.
Weather event | Communication | Study type | Effectiveness |
|---|---|---|---|
“natural disasters”; “flood risk”; Flood*; drought; Heat; Cold | Risk perception; Perception* | “systematic review”; “literature review”; “evidence review” | Evaluation; effectiveness |
Table 2: Question 3 search terms
Inclusion and exclusion criteria
We established a two-tiered set of primary and secondary criteria to guide the search and screening process. The primary criteria were designed to ensure that initial retrieval was relevant to the study’s focus, while the secondary criteria were applied during the abstract and full-text review stages to assess relevance and quality in greater depth. These are shown in Table 3 below.
Primary criteria defined the parameters of relevance across four domains:
Weather event type: studies addressing heat, cold, flooding, or drought.
Geographic scope: we prioritised studies focusing on Scotland and the wider UK, alongside research from comparable international contexts, defined as high-income countries with institutional capacity for public health communication, broadly similar exposure to climate-related weather risks, or temperate climates. These were: North America, Western and Northern Europe, Australia, and New Zealand.
Language: English only.
Publication period: 2015–2025. We selected the starting point of 2015 to balance breadth and relevance within the constraints of a rapid review methodology. The date range reflects the growing research focus on climate resilience over the past decade, while ensuring the volume of literature remained manageable and timely for synthesis.
Where database functionality permitted, we embedded some of these parameters (language and publication date) directly into the search filters to ensure precision and relevance from the outset. These same criteria were then used to exclude clearly out-of-scope titles (for example, papers on unrelated hazards).
We developed secondary criteria to screen abstracts and full-texts. These captured both substantive relevance (how well the study aligned with the research aims and scope) and quality (how robustly the evidence was generated or reported). To support consistency and transparency, each record was assigned a numerical score for each criterion (0 = absent; 1 = partially present; 2 = fully present), producing a weighted, transparent system for prioritising inclusion. Records with the highest cumulative scores were retained for synthesis. Geography was included again among the secondary criteria to allow prioritisation of studies conducted in Scotland or the wider UK.
Inclusion | Exclusion | |
|---|---|---|
Primary search criteria and title screening | ||
Type of adverse weather event | Four weather events in scope (drought, flooding, heat, cold) | All other hazards |
Geographic location | Scotland/UK and comparable countries (USA and Canada, Australia, New Zealand, Northern / Western Europe) | Studies focused only on other regions |
Language | English | Publications in any other languages |
Timeframe | 2015-2025 | Outside of this date range (unless highly relevant / influential publication) |
Secondary search criteria for abstract screening and full-text review | ||
Geographic location | Scotland/UK and comparable countries (USA and Canada, Australia, New Zealand, Northern / Western Europe) | Studies focused only on other regions |
Health outcomes | Addresses health protective knowledge, awareness, behaviour or health impacts | Does not address health outcomes |
Presence of messaging example | Includes example of a message | Does not include a messaging example |
Disaster management cycle (DMC) | Can be linked to preparation, response or recovery | Cannot be linked to these three phases of the DMC. |
Study quality | Demonstrates innovation, effectiveness, or replicability (if the study was a specific communication ‘intervention’), liked to our evidence framework and/or strong conceptual framing, methodological transparency, and validity (further details in Quality Appraisal below) | Study is of poor quality |
Table 3: Inclusion and exclusion criteria
Quality appraisal
Our appraisal approach reflected the potentially diverse nature of the evidence base, encompassing both ‘intervention-focused’ studies (for example, those describing or testing a messaging strategy or design, or a communications campaign) and studies that may draw conclusions about the nature and approach to messaging based on empirical data or evidence reviews. All studies were assessed using a core set of quality criteria, covering:
Conceptual framing: whether the study articulated a clear conceptual framework or research question, and whether conclusions were grounded in empirical evidence.
Methodological transparency: whether the research design and methods were described, and whether data sources were clearly cited or traceable
Validity: whether the study demonstrated internal validity (e.g. consideration of alternative causes or limitations) and external validity (e.g. generalisability to other contexts or populations).
For ‘intervention-focused’ studies, these criteria were supplemented with an Evidence Effectiveness Framework (Cullen, J et al., 2019) – a Standards of Evidence tool developed by the research team to assess the strength of evidence in emerging policy areas where few interventions have been evaluated through experimental methods such as RCTs. The framework, derived from a review of 19 major standards-of-evidence scales, applies tight criteria and categorises interventions as innovative, effective, or replicable. For instance, replicability denotes that an intervention (such as a campaign) has been robustly evaluated or has demonstrated transferable results in comparable contexts.
We scored each quality component (conceptual framing, methodological transparency, validity) using the scoring system described above (0–2 scale) and calculated the average quality score. This was then combined with relevance criteria (e.g. geography, presence of messaging, link to the disaster management cycle) to form the total weighted score used in shortlisting.
Piloting
We conducted a piloting stage to test the sensitivity and precision of the draft search strings across the originally selected databases — PubMed, ProQuest, and Google/Google Scholar. The pilot returned a high number of low-relevance results from Google searches, which informed our decision to reorient the search strategy: we added Web of Science as a third database to strengthen coverage of peer-reviewed literature and limited the use of Google to targeted grey-literature searches at a later stage (during abstract and full-text review).
During this piloting phase, we retained all records that appeared potentially relevant. Several of these early items were grey-literature reports, which we kept on a provisional list for consideration in the subsequent targeted grey-literature search.
Piloting also confirmed the need to adapt search syntaxes and Boolean combinations for each database to ensure optimal retrieval of relevant records, as platforms varied in how they indexed and parsed search terms.
As an additional quality assurance step, we used Medical Subject Headings (MeSH) on Demand in PubMed to confirm that our search strategy was retrieving all relevant studies. The tool analyses the abstract and keywords of an article to identify similar papers and their associated key terms. We applied this process to several relevant papers identified during the pilot search across weather events to check whether additional studies were retrieved, and to identify any additional terms that could refine our search strings. This exercise confirmed that our search strategy captured the core evidence base.
Stage 2: Formal search and longlisting
We conducted the formal search using the finalised search strings across the three databases. All records were then exported into a bibliographic spreadsheet in Microsoft Excel, containing key fields (authors, year, title, source, and abstract). This enabled the review team to carry out title screening (described in more detail below) directly within the spreadsheet to remove studies clearly out of scope according to the primary inclusion criteria. We also developed an additional structured matrix specifically for this evidence review to include both the primary and secondary criteria. All records that passed title screening were transferred into the matrix and also exported into Zotero reference-management software, which provided the foundation for subsequent abstract and full-text screening and scoring. This structure ensured a consistent, transparent, and auditable workflow, allowing reviewers to record inclusion decisions and quality scores systematically.
Stage 3: Screening and shortlisting
The screening followed a three-tier process based on titles, abstracts, and full texts against inclusion and exclusion criteria.
Tier 1 – Title screening: focused on removing items that databases captured but were clearly out of scope. Examples included records outside the four weather events in scope (such as COVID-19), or that focused on general climate adaptation policy or environmental health studies. If a title did not make its relevance clear, the paper was retained for Abstract screening rather than excluded.
Tier 2 – Abstract screening: we reviewed and scored Abstracts against the inclusion and exclusion criteria. Records that appeared ambiguous were either flagged for second-reviewer discussion or retained for full-text screening to avoid premature exclusion. For example, studies mentioning alert systems but potentially containing relevant communication insights or learning were retained for full-text screening.
Tier 3 – Full-text screening: The remaining items were reviewed in more depth looking at the full texts, again against the secondary inclusion criteria.
In parallel, we conducted a targeted second-wave search for grey literature. This built on the provisional list of items identified during the piloting phase.
Two reviewers conducted all screening activities independently. We held regular meetings to discuss and resolve any discrepancies, with final adjudication resolved through discussion and consensus and quality-assurance oversight, provided by the project director. Studies achieving the highest cumulative scores were retained for data extraction.
Throughout the process, we maintained flexibility in applying the scoring framework, recognising that few studies offered formal evaluations of communication interventions. For example, we retained high-quality studies conducted in other regions (e.g. Japan) where evidence offered strong empirical insights, and we also included studies focused on alert or warning systems (which were out of the scope of the research) where the communication elements demonstrated transferable lessons for public-health messaging.
Selection of sources of evidence
Using 15 search strings adapted for three databases (Web of Science, PubMed, ProQuest), we screened 3,568 titles. Following the initial title screening, 3,225 records were excluded.
This left 343 records sought for retrieval. Within this group, 127 duplicate records were removed, and the 68 relevant reports identified during the pilot searches were added, resulting in a total of 284 records that were assessed at the abstract screening stage. A total of 48 studies proceeded to full-text screening, during which 20 were excluded. This process yielded 28 peer-reviewed studies included in the synthesis.
The targeted grey-literature search identified 13 candidate reports. After appraisal, five were retained. We excluded items that were outside the date range (2013), two (on flooding and drought) because they duplicated material already captured through peer-reviewed studies, and others (mostly heat-related) because stronger evidence had already been included. The final sample comprised 32 studies (26 peer-reviewed articles and six grey-literature reports) taken forward for extraction and synthesis. The full process is illustrated in the PRISMA flow diagram below.
Figure 1 PRISMA flow diagram
Data extraction and synthesis
We extracted information from each item using a structured template developed in Microsoft Word (see Appendix B). The template was organised around the study’s three research questions and drew on established knowledge on the components of effective communication and on the factors influencing risk perception and behaviour, as summarised in existing frameworks (e.g. Fathollahzadeh et al., 2023; Spielhofer et al., 2020). This provided the conceptual framework for the analytical process.
To ensure consistency and fitness for purpose, each member of the research team piloted the template using three literature items that reflected slightly different types of evidence (an evidence review, an empirical study, and an evaluation of an intervention). We made minor refinements to harmonise interpretation of fields, accommodate the diversity of the studies, and to streamline the information.
We then imported the extraction templates into MAXQDA, a qualitative analysis software that enabled systematic coding and synthesis of themes across the evidence base in line with the three research questions.
Engagement Phase
Phase 2: Engagement
The aim of this phase was to engage with organisations representing groups particularly at risk of negative health impacts of adverse weather in Scotland and / or hard to reach. We carried out five workshops and four interviews to explore barriers, motivators and enablers to engagement and participation in adverse weather health messaging.
Three workshops were with organisations representing parents / carers of young children under 5; ethnic minority communities; older adults and adults with particular health conditions.
Two workshops were place-based, focused on Glasgow Easterhouse and Dumfries and Galloway, designed to explore lived experiences of specific weather events, the kinds of messaging people had seen or received, and what types of communication worked best in their context. We selected Dumfries due to its frequent flooding, linked to proximity to the River Nith. We selected Glasgow as an urban setting for insights on heat and cold, where high social vulnerability (for example related to poor housing) can limit people’s ability to prepare for and respond to temperature extremes.
Four one-to-one semi-structured interviews were carried out with representatives of specific communities. These were the Gypsy Traveller community; organisations working with minoritised communities; place-based experience of flooding (Dumfries and Galloway); and Water Safety Scotland (flooding, extreme heat and cold).
The insights gathering process for Phase 2 was conducted from September and October 2025. Through online interactive workshops and interviews we explored the barriers, motivators, and enablers shaping engagement with adverse-weather messaging.
We conducted:
3 organisational workshops (Early Years, Health/Age, Diverse Communities)
2 place-based workshops (Glasgow Easterhouse, Dumfries and Galloway)
4 semi-structured interviews
We spoke to:
22 people
13 organisations
3 communities
Organisation list:
- Early Years
- Safety
- Health/Age
- Diverse Communities
- Place-based
- Pavillion
Community councils in Dumfries and Galloway
- Pavillion
Workshop Guide and Materials
The template workshop guide used for each workshop is as follows. Note that each workshop was tailored to fit the adverse weather events spoken about, and public health materials discussed, depending on the population group spoken to. Each workshop was between an hour and an hour and a half.
Workshop guide – Organisational workshops
Timings | Activity |
5 mins | Welcome and introductions
Ask participants to introduce themselves: name, org, and location, size of organisation and who they work with Welcome into the space, pop name, org, and favourite season in the chat |
10 mins | Introduction Thanks again to you all for joining this session. Before we jump into the session we’ll give you a little more information on the project and why we’re here today. We are working with ClimateXChange, who are Scotland’s centre of expertise on climate change, to figure out the best ways to communicate nationally about healthy behaviours before, during, and after adverse weather. This involves both the message content and the communication channels used. The findings of this research will help to support delivery of the Public Health Scotland’s Adverse Weather and Health Plan, which sets out how PHS, with support from the Scottish Government and working in partnership with key stakeholders, will help to protect Scotland’s health from adverse weather-related harm. Now when we talk about adverse weather, we mean extreme weather, which is becoming more common with climate change. For the purpose of this project we’re focusing on extreme heat, cold, flooding, and drought. And while extreme weather affects everybody, we know that there are certain groups of people that can be more at-risk than others. This is why we’ve reached out to you – [insert rationale here] We’re here to understand how this population group reacts to different kinds of adverse weather, and what kinds of messaging work best, and we’ll be doing this through a series of questions and discussion today. Space for questions
We’d like to ask for consent to record this workshop, purely for notetaking purposes and to share with our data team. Does everyone consent? START RECORDING IF SO Now let’s head to Miro to begin. Does everyone know how to use Miro? Explain if not |
20 mins | Activity 1 – experiences with adverse weather Learning question: What factors influence the public’s risk perception and health and wellbeing behavioural responses in relation to adverse weather events? Purpose: understanding how population group are affected by adverse weather We know that often people’s responses to bad weather depend on their past experiences, how much they trust warnings, what they understand about the risk, what resources they have, and the support from their community. We want to understand more about how your population group respond to bad weather – like heatwaves or flooding – depends on their past experiences, how well they understand the risks, the support they have, and whether they can get what they need to stay safe and healthy. We also want to understand how you as an organisation support them either directly or through information that you share. Activity: Matrix with 4 adverse weather types, with spaces for intersection “Think about the [population group] you work with (either directly or indirectly). For the weather events you’ve had experience with, what has been this group’s perception/ experience?” Prompts: were they worried or not concerned? Were they prepared or not? Did they experience a challenge? Why? Risks: Did you feel that the people you work with or share information with understand the risk? If yes – how do you know? Prompts for stories |
20 mins | Activity 2 – experiences with public health messaging of adverse weather Learning question: Which communications channels used for adverse weather events (for general and at-risk populations) are most effective and why? Purpose: understand how population group respond to public health messaging Now we’re going to focus on public health messaging and explore how your population group has responded to it in the past, to understand what works, what doesn’t, and what could be made better. We asked you to bring in any examples of messaging that you may have used (it could have been for these 4 main weather events, but could be general messaging around weather, or health related) – if anyone has them handy could you share it with us and tell us a bit about it? Prompts: What have you done in face of adverse weather events with messaging? Where do you go to get your advice? Where/how/what made the messaging stick? What was the content? What were channels x delivery? What could make it more effective? Discussion + record points on Miro Now we’re going to share some public health messaging we found (it may be the same or different). Have you used any of these sources for information? What makes them effective/not effective for your population group? Why/why not? Have they or how have they used messaging from PHS, or do you use or pay attention to other organisations around adverse weather messaging and why? |
20 mins | Activity 3 Based on our discussions today, our last activity will pull this all together and explore what public health messaging should include and how it should be delivered. We’ve created a very rudimentary piece of messaging here: based on what we’ve discussed, what would you choose to include, why and how? |
10 mins | Discussion / Reflections – on key themes discussed |
5 mins | Next steps and thank you Thank you very much for your time today. We will take away all this information, analyse it and pull together recommendations on how to make public health messaging more effective for your population group and the others we are focusing on. If you think of anyone else who may be interested in joining a workshop or interview, please email me. Have a good rest of the day/evening! |
Workshop guide – Place-based workshops
Timings | Activity |
5 mins | Welcome and introductions Welcome people into the space, ask them to pop their name, and favourite season in the chat |
10 mins | Introduction Thanks again to you all for joining this session. Before we jump into the session we’ll give you a little more information on the project and why we’re here today. We are working with ClimateXChange, who are Scotland’s centre of expertise on climate change, to figure out the best ways to communicate nationally about healthy behaviours before, during, and after adverse weather. This involves both the message content and the communication channels used. The findings of this research will help to support delivery of Public Health Scotland’s Adverse Weather and Health Plan, which sets out how PHS, with support from the Scottish Government and working in partnership with key stakeholders, will help to protect people’s health in Scotland from adverse weather-related harm. Now when we talk about adverse weather, we mean extreme weather, which is becoming more common with climate change. For the purpose of this project we’re focusing on extreme heat, cold, flooding, and drought. And while extreme weather affects everybody, we know that there are certain places that may experience the effects more than others. This is why we’ve reached out to you and your community – we know through research that [insert place and rationale] We’re here to understand your experience during periods of extreme heat and cold, what kinds of messaging you’ve seen or received about extreme heat and cold, and what messaging works best. We’ll be doing this through a series of questions and discussion today. Space for questions
We’d like to ask for consent to record this workshop, purely for notetaking purposes and to share with our data team. Does everyone consent? |
20 mins | Activity 1 – experiences with adverse weather Think about the last time you experienced [insert adverse weather type]. What was it like? Were you worried or not concerned? Were you prepared or not? Did you experience a challenge? What helped you get through it? What support did you have? If you haven’t experienced either weather event, do you feel prepared for it? |
25 mins | Activity 2 – experiences with public health messaging of adverse weather Now we’re going to focus on public health messaging, to understand what works, what doesn’t, and what could be made better. When we talk about public health messaging, we mean any sort of communication sent out that is aimed to inform people about an event, risk, or thing related to health, so that people can make informed choices to prepare themselves and stay healthy. These messages might be posters, text alerts, letters, emails, or ads. We’ve got a couple examples from PHS on extreme weather here. (Show examples of public messaging here) Can you think of any public health messaging that you’ve seen related to [insert adverse weather type]? If yes – what was it, and how was it sent to you? Did it help you, or not? Why? If no – what have you used instead, and how did you find it? Was it helpful? Why? Discussion + record points on Miro Now we’d like to ask how you share information in your communities. In your communities, what ways do you share information about extreme weather? For example, WhatsApp chats, bulletin boards Have you shared any information with friends/family/your wider community to help prepare them? Have they shared anything with you? Discussion + record points on Miro |
20 mins | Activity 3 Based on our discussions today, our last activity will pull this all together and explore what public health messaging should include and how it should be delivered. We’ve created a very rudimentary piece of messaging here: based on what we’ve discussed, what would you choose to include, why and how? What would make messaging more effective for your local community, both in content and how to share it? |
5 mins | Discussion / Reflections – on key themes discussed |
5 mins | Next steps and thank you Thank you very much for your time today. We will take away all this information, analyse it and pull together recommendations on how to make public health messaging more effective for everyone. |
Interview Guide
Find below the interview guide template used for semi-structured interviews. Interviews were around 45 minutes long, conducted online.
Introduction
Thank you for taking the time to participate in this interview. Before we jump into the interview I’ll give you a little more information on the project. We are working with ClimateXChange, who are Scotland’s centre of expertise on climate change, to figure out the best ways to communicate nationally about healthy behaviours before, during, and after adverse weather. This involves both the content of the message and the communication channels used.
The findings of this research will help to support delivery of the Public Health Scotland’s Adverse Weather and Health Plan, which sets out how Public Health Scotland, with support from the Scottish Government and working in partnership with key stakeholders, will help to protect people’s health from adverse weather-related harm.
Now when we talk about adverse weather, we mean extreme weather, which is becoming more common with climate change. For the purpose of this project we’re focusing on extreme heat, cold, flooding, and drought. And while extreme weather affects everybody, we know that there are certain groups of people that can be more at-risk than others.
This is why we’ve reached out to you – [insert rationale here]
GAIN CONSENT TO RECORD THE SESSION
Tell me about a recent flood, drought, heatwave, or bout of extreme cold that impacted your population group. Did they see the event as a risk, or did they feel prepared? Do you know what their reaction was afterwards? Were they influenced into action, and how?
**Note: If they haven’t experienced any of these four, broaden to any adverse weather event
Related to the weather example you’ve just told me, which communication channels do you believe were most effective for reaching your population group, and why? Which do you think were least effective?
How does your organisation approach their comms when it comes to relaying a public health message around adverse weather?
Prompts: what considerations / principles inform their approach to:
-
content (tone, clarity, type of information, quantity, language considerations)
format (visuals etc).
any differences by weather event?
differences by stage (before, during, after a weather event)
Thinking about content, what do you think works best when relaying an effective public health message? Why?
What do you do with your messaging to reach and engage the people that you represent/the people you want to see this messaging?
Prompts: highlight what is communicated (message design, content) and how (e.g. channel, dissemination strategy), and when (before a weather event, during, after)
What are the main barriers your population group face in engaging with health messages about weather-related risks?
What are the key enablers that help your population group engage with and act on health messages about adverse weather?
As a result of the struggles/challenges/barriers, have you seen an increase in awareness/knowledge/motivation to change their attitudes or behaviours in the face of an adverse weather event?
Research scope
The research was designed to examine how communication can support protective health behaviours in response to adverse weather events (heat, cold, flooding, and drought). The review focused on what is communicated, how messages are delivered, and the factors that influence whether people engage with public health messaging.
As a result, some related issues were outside the scope of this research. For example, we did not examine the role of misinformation or disinformation in shaping public responses to adverse weather and this did not emerge as a prominent theme in the literature identified with the help of our search criteria. However, this is an important area of concern, particularly in the context of social media, and we note it as an area for further exploration. For readers seeking additional insight, relevant developments can be found in the Scottish Health Information Integrity Strategy 2025-2030 (Scottish Government, 2025).
Section 1: Basic item information This section captures basis information on the scope and focus of the item reviewed. | |
|---|---|
Full item details: Title, author(s), link to publication, DOI. | |
Item type | Indicate the type of study the item represents: Scoping review Lit Review Systematic review Empirical study Evaluation Other Please specify: |
Type of adverse weather event covered | Tick the type of adverse weather event covered. If multiple events, tick all boxes that apply: Flooding Heat Drought Cold Multiple events Please specify which adverse weather events are covered: |
Focus of the item | Tick all that apply: Public health messaging Message example Communication channels General Population At risk population Specify which at risk population is studied:
Health and wellbeing behavioural responses Health outcomes Specify which health outcomes are included: Risk perception |
Geographic location | Indicate which geographic location the item focuses on: Scotland England UK Northern Europe Western Europe North America Australia New Zealand Other Please specify: |
Stage of emergency management cycle | Indicate which stage of the emergency management cycle the item discusses: Preparation (before) Response (during) Recovery (after) |
Article summary | Create a short summary of what the publication is about. Include aim of the research and key findings. |
Methodological design | Provide a brief summary of the study’s design. Include the research questions and its overarching conceptual framework. Summarise type of evidence generated (qualitative, quantitative, mixed methods) and key methods used. Add any limitations to the study highlighted by the authors. Conceptual frame: Methodology: Research questions: |
Strength of evidence assessment | Does this item present research or evaluation of a specific ‘intervention’ (e.g. a message or communication strategy)? Yes (complete the strength of evidence assessment below) No (go to section 2) |
If answered yes to the question above: using the Medici strength of evidence framework, make a judgement on how strong the evidence on the effectiveness of the public message examined is. Innovative Effective Replicable Provide a rationale for this assessment: | |
Section 2: Evidence on the study’s three research questions This section summarises the evidence presented by the item in relation to the three research questions covered by the review | |
RQ 1. (WHAT) | Summarise the key findings articulated in the item on whether and how public health messages / messaging have / has been successful in encouraging health protective behaviours among the groups investigated. Explain what heath protective behaviours have been encouraged and whether the item links them to wider health outcomes (and which ones). If the item investigates the impact of a specific health message, please include this below. |
(HOW / WHY?) | Does the article consider the role of the audience’s external context when analysing the impact on health protective behaviour of the public health messaging? External context covers the spatial, cultural and temporal dimensions within which the target audience is situated (such as their social and other capital, power structures and trust in authorities, the audience’s relationship to the physical space) Yes No If yes, summarise what external context factors were considered and how they were seen to influence the effectiveness of the public health message / messaging investigated. Spatial context: Temporal context: Trust in authorities: |
(HOW / WHY?) | Does the article consider factors related to the population’s propensity to change behaviour when discussing / explaining changes in health behaviours? This includes: Audience characteristics: including prior experience of the hazard, proximity (temporal or spatial) to the hazard, connection to place, socio-cognitive factors: the extent to which social norms, belief in self-efficacy, values and fear influence risk perception and propensity to act. Demographic characteristics Yes No If yes, summarise what factors were considered and how these were seen to influence behavioural responses to public health messaging. Audience characteristics: Socio-cognitive factors: Demographic characteristics: |
RQ 2. (WHAT?) | Summarise the key findings of the article on the most effective communication channels for public health messaging on adverse weather events (for general and / or at-risk populations). Include why the channel(s) are considered (most) effective. Include, where applicable: the communication channels discussed data on effectiveness of these channels (e.g. reach, link to behaviour change). |
(HOW / WHY?) | Does the article discuss the link between message content and audiences’ behaviour changes? This includes style of message and nature of message (e.g. action focused, information focused). Yes No If yes, summarise key findings: |
(HOW / WHY?) | Does the article analyse the relevance of who sent the message and where the message originated (message sender and source, including questions of trust) in relation to any behaviour change outcomes observed? Yes No If yes, summarise key findings: |
Any other information | Add any other information relevant |
Key relevant lessons | |
Geographical coverage | Weather event | Study design/method | RQ | |
|---|---|---|---|---|
Antwi, S.H., Rolston, A., Linnane, S. and Getty, D., (2022). Communicating water availability to improve awareness and implementation of water conservation: A study of the 2018 and 2020 drought events in the Republic of Ireland | Republic of Ireland | Drought | Study analysing public communication on drought and water conservation, combining content analysis of social media posts (Twitter and Facebook) and newspaper coverage with six interviews with journalists, political representatives, and water and communication experts. | 3 |
British Red Cross (2023): Policy Brief: public perceptions of heatwaves in the UK | UK | Heat | Nationally representative survey (UK) of public perceptions of heatwaves. | All |
Bourret Soto, M. and Guillon, M., (2024). What drives adaptive behaviours during heatwaves? A systematic review with a meta-analysis. | Asia, North America, Oceania, Europe | Heat | Systematic Review of existing quantitative evidence on the determinants of health protective behaviours in the face of heatwaves. Examined how psychological (efficacy, knowledge, risk, threat), demographic (age, gender, socio-economic status), and health status influence adoption of heat-adaptive behaviours. | 3 & 1 |
Bruine de Bruin, W., Lefevre et al., 2015, C.E., Taylor, A.L., Dessai, S., Fischhoff, B. and Kovats, S., (2016). Promoting protection against a threat that evokes positive affect: The case of heat waves in the United Kingdom. | UK | Heat | Online experiment testing whether recalling past unpleasant temperatures was linked to intention to take up health protective behaviours. Specifically, to examine whether recalling different types of past temperatures (pleasant/unpleasant, high/low) could shift risk perceptions and behavioural intentions. | 3 & 1 |
Coombs, N.M., Porter, J.E. and Barbagallo, M., (2024). An exploration of the influencing factors for effective public health messaging during disasters: a scoping review. | North America, Australia, Asia | Mix (including flooding) | Scoping review to explore how public health messages are currently being provided during disasters and identify what influencing factors contribute to the effectiveness of these messages. | All |
Erens, B., Williams, L., Exley, J. et al. (2021): ‘Public attitudes to, and behaviours taken during, hot weather by vulnerable groups: results from a national survey in England’. | England | Heat | Analysis of nationally representative survey of adults (England) supplemented with four focus groups with older adults. | All |
Esplin, E.D., Marlon, J.R., Leiserowitz, A. and Howe, P.D. (2019). “Can you take the heat?” Heat-induced health symptoms are associated with protective behaviours. | Phoenix, Arizona (USA) | Heat | Study used national survey data linked to local temperature conditions and analysed whether people who were exposed to extreme heat or had experienced heat-related health effects were more likely to take protective actions. | 3 & 1 |
Fathollahzadeh A, Salmani I, Morowatisharifabad MA, Khajehaminian MR, Babaie J, Fallahzadeh H. (2023). Models and components in disaster risk communication: A systematic literature review. | Asia, USA, Europe | Mix (including flooding) | Systematic review to identify and classify influential components in risk communication (message, message sender, message receiver, message environment, message process) | All |
Forsyth, W., Roberts, T., & Brewer, G. (2023). Conceptualising risk communication barriers to household flood preparedness. | Primarily Europe | Flooding | Systematic review on risk communications and household flood preparedness. | All |
Global Water Partnership (2019). ‘How to communicate Drought: a guide by the Integrated Drought Management Programme in Central and Eastern Europe’. | Central/Eastern Europe | Drought | Guide setting out principles and practices to communicate drought, compiled by an international network of 12 Country Water Partnerships (Integrated Drought Management Programme Central and Eastern Europe). Based on available literature and expertise of partnership stakeholders. | 3 |
Health Canada (2011; updated in 2020). ‘Communicating the Health Risks of Extreme Heat Events: Toolkit for Public Health and Emergency Management Officials’. | Canada | Heat | A good practice toolkit setting out recommended communication approaches for addressing health risks from extreme heat. Draws on experience from Canadian and international contexts, informed by expert input and a review of the existing literature. | All |
Henderson, F., Helwig, K. and Teedon, P., (2022). Effective future communication of flood risk in Scotland. | International, and Scotland-specific | Flooding | Rapid Evidence Assessment, supplemented with interviews and workshops with stakeholders with lived experience and professional insight in communicating and/or acting on flood risk in Scotland. | All |
Lefevre, C.E., Bruine de Bruin, W.B., Taylor, A.L., Dessai, S., Kovats, S. and Fischhoff, B., (2015). ‘Heat protection behaviours and positive affect about heat during the 2013 heat wave in the United Kingdom’. | UK | Heat | UK-wide, non-representative survey of adults, with deliberate over-representation of older adults. | All |
Li, Y., & Howe, P. D. (2023). ‘Universal or targeted approaches? An experiment about heat risk messaging’. | USA | Heat | Online, randomised survey-based experiment to examine how best to communicate susceptibility to heat-health risks in messaging aimed at the general public, by comparing four message variations: listing only vulnerable groups, stating that “anyone can be at risk,” combining both, or using a neutral explanation. | 1 & 3 |
Li, Y., Hughes, A.L. and Howe, P.D., (2018). ‘Communicating Crisis with Persuasion: Examining Official Twitter Messages on Heat Hazards’. | USA | Heat | Content-analysis of heat-related Twitter messages (N=904) posted by eighteen U.S. National Weather Service Weather Forecast Offices. | All |
McClymont, K. and Beevers, L. (2022). ‘Understanding the social factors influencing resilience to drought exposure in Scotland’. | Australia, Africa, Asia, South America, Europe, with specific applications to Scottish context | Drought | Systematic review of international evidence on the personal, social, environmental, and institutional factors (conversion factors) that shape drought vulnerability and application of findings to drought communication in Scotland, particularly for communities on Private Water Supplies (PWS). | All |
MacIntyre E, Khanna S, Darychuk A, Copes R, Schwartz B (2019): ‘Evaluating risk communication during extreme weather and climate change: a scoping review’. | Primarily North America and Europe | Mix (including flooding and heat) | Scoping review on effective communication to inform public health messaging regarding climate change and extreme weather (supplemented by expert/stakeholder consultation workshops) | All |
McLoughlin, N., Howarth, C. and Shreedhar, G., (2023). ‘Changing behavioural responses to heat risk in a warming world: How can communication approaches be improved?’ | Asia, North America, Europe (including UK) | Heat | Scoping review of behavioural and attitudinal studies about heat risk responses to inform communication approaches. | All |
Mehiriz, K., Gosselin, P., Tardif, I., & Lemieux, M. A. (2018). ‘The effect of an automated phone warning and health advisory system on adaptation to high heat episodes and health services use in vulnerable groups – evidence from a randomized controlled study’. | Canada | Heat | Randomised Controlled Trial to measure the (behavioural and health) effects of an automated phone warning and advisory system on people vulnerable to heat. Three surveys: an initial survey on demographic/socioeconomic characteristics after recruitment; a baseline survey on outcome measures; a final survey after the heat warning on outcome measures | 1 |
Nitschke M, Krackowizer A, Hansen AL., Bi P, Tucker GR (2017): ‘Heat Health Messages: A Randomized Controlled Trial of a Preventative Messages Tool in the Older Population of South Australia’. | South Australia | Heat | Randomised Controlled Trial. The intervention was an information package (an information sheet on how to deal with extreme heat; a laminated top tips card; fridge magnet; the local health authority’s Extreme Heat booklet; three fact sheets) with a control group advised to take notice of public announcements, messages. Data collected through three surveys | 1 & 2 |
Oakman, T., Byles‐Drage, H., Pope, R., & Pritchard, J. (2010). ‘Beat the Heat: don’t forget your drink–a brief public education program’. | New South Wales, Australia | Heat | Cross-sectional survey measuring self-reported awareness, knowledge, and behaviours related to heat stress following a public health communication campaign. | All |
Olson, M. K., Sutton, J., & Waugh, N. (2023). ‘Tweeting the Heat: An Analysis of the National Weather Service’s Approach to Extreme Heat Communication on Twitter’. | USA | Heat | Quantitative content analysis of 250 tweets from seven National Weather Service forecast offices during a major heat event, coding messages for hazard framing, impacts, guidance, and references to vulnerable populations. | All |
Ratwatte, P., Wehling, H., Kovats, S., Landeg, O., & Weston, D. (2022). ‘Factors associated with older adults’ perception of health risks of hot and cold weather event exposure: a scoping review’. | North America, Europe (including UK), Australia | Heat/cold | Scoping review on factors influencing behaviours and risk perception for hot and cold weather (older adults) | 1 & 3 |
Takahashi, N., Nakao, R., Ueda, K., Ono, M., Kondo, M., Honda, Y., & Hashizume, M. (2015). ‘Community trial on heat related-illness prevention behaviors and knowledge for the elderly’. | Japan | Heat | Quasi-experimental study | 1 |
Tan, H., Hao, Y., Yang, J. and Tang, C., (2024). ‘Meta-analyses of motivational factors of response to natural disaster’. | Mix (including flooding) | Meta-analyses of motivational factors influencing individuals’ behavioural responses to natural disasters | All | |
Tetzlaff, E.J., MacDonald, M., Kenny, G.P., Murphy, B., Siblock, R.F., Al.-Hertani, A., Stranberg, R.C., Berry, P. and Gorman, M., (2025a). ‘Updating Health Canada’s Heat-Health Messages for the Environment and Climate Change Canada Heat Warning System: A Collaboration with Canadian Experts’. | Canada | Heat | The study combined a review of recent evidence on heat events with structured input from public health and climate experts, readability testing, and equity checks to iteratively refine and prioritise heat-health messages for use in short-form public messaging. | All |
Tetzlaff, E. J., Wagar, K. E., Johnson, S. J., Gorman, M., & Kenny, G. P. (2025b). ‘Heat-health messaging in Canada: A review and content analysis of public health authority webpages and resources’. | Canada | Heat | Qualitative content analysis of heat-health information on public health websites using descriptive coding to identify how risks, vulnerable populations, and protective actions were communicated. | 2 |
Turner, G.A., Moreira de Sousa, A., O’Connell, E., Kovats, S., Brooks, K., Landeg, O., Ismail, S., Rajamani, A. and Hajat, S., (2024). ‘Health perceptions of adverse weather in older adults in England: analysis of 2019/20 survey data’. | England | Heat/cold | Used nationally representative survey data from older adults in England to examine perceptions of the health risks associated with hot and cold weather, and explore factors associated with these perceptions and related protective behaviours. | 1 & 3 |
VanderMolen, K., Kimutis, N. and Hatchett, B.J., (2022). ‘Recommendations for increasing the reach and effectiveness of heat risk education and warning messaging’. | San Diego, CA (USA) | Heat | Qualitative study with 43 individuals representing or serving heat-vulnerable communities (community leaders, nonprofit reps, local government, healthcare, educators, utilities), with results considered in light of broader evidence of good practice. | All |
Vu, A., Rutherford, S. and Phung, D., (2019). ‘Heat health prevention measures and adaptation in older populations—a systematic review’. | Australia, Europe, North America, Japan | Heat | Systematic review on risk factors awareness, perception of vulnerability, and protective behaviours of older people against existing government-issued mitigating measures in the events of heatwaves. Includes professional and non-professional personnel responsible for the health and welfare of older people. | 3 & 2 |
Weitkamp, E., McEwen, L. and Ramirez, P., (2020). ‘Communicating the hidden: Toward a framework for drought risk communication in maritime climates’. | UK | Drought | Co-produced, mixed-methods study based on engagement (participatory workshops and interviews and input from a national stakeholder group) with local advisory groups across seven UK catchments and, supplemented by in-depth interviews with statutory and non-statutory stakeholders. | 2 & 3 |
Williams, L., Erens, B., Ettelt, S., Hajat, S., Manacorda, T. and Mays, N., (2019). Evaluation of the heatwave plan for England. | England | Heat | Mixed methods evaluation of the heatwave plan for England. | All |
How to cite this publication:
Iacopini, G; Junge, K; Drabble, D; Owen, C Tombazzi, A. (2026) ‘Effective public health messaging for adverse weather events’, ClimateXChange. https://doi.org/10.7488/era/7268
© The University of Edinburgh, 2026
Prepared by The Tavistock Institute of Human Relations and Innovation Unit on behalf of ClimateXChange, The University of Edinburgh. All rights reserved.
While every effort is made to ensure the information in this report is accurate as at the date of the report, no legal responsibility is accepted for any errors, omissions or misleading statements. The views expressed represent those of the author(s), and do not necessarily represent those of the host institutions or funders.
This work was supported by the Rural and Environment Science and Analytical Services Division of the Scottish Government (CoE – CXC).
ClimateXChange
Edinburgh Climate Change Institute
High School Yards
Edinburgh EH1 1LZ
+44 (0) 131 651 4783